




Clinical Practice As an Engine Driving a Translational Research Program in Pancreatic Cancer
Eugene P. Kennedy*1, Jonathan R. Brody1, Agnes Witkiewicz2, Harish Lavu1, Patricia K. Sauter1, Dane Grenda1, Dianne Macrae1, Florence Williams1, Ernest L. Rosato1, Charles J. Yeo1
1Surgery, Thomas Jefferson University, Philadelphia, PA; 2Pathology, Thomas Jefferson University, Philadelphia, PA
Objective: Traditionally, clinical and research pursuits have occurred in parallel. In the current climate of reduced research funding and increased need for translation of discoveries, an integrated program is an appealing strategy. This study was designed to demonstrate research benefits of a robust clinical practice.Methods: Review of our database revealed a total of 1005 pancreatic resection for the period January 1, 1995 through December 31, 2009 (annualized). The period January 1, 2006 onwards included 711 pancreatic resections and was correlated with research activities. Results: The growth in pancreatic resections produced professional fees averaging $3500/case to Surgery and $3000/case to other departments. Hospital contribution margin averaged $13500/case. The increased pancreatic resection volume has contributed more than $3 million annually to the positive hospital bottom line.Since 2006, 5 randomized clinical trials and 3 approved protocols have opened. Tissue and plasma on greater than 400 patients has been banked. 37 peer reviewed publications have resulted. The research team now numbers 23 independent researchers from our institution and 34 independent researchers from 16 collaborating institutions. Patient participation in protocols is high, from 95% on our tissue banking protocol to 74% on our recent published pancreatic anastomosis trial.Conclusions: Building a robust clinical practice can drive a complementary research program. Clinicians in leadership roles in the effort can drive productivity, extensive collaboration, and high patient participation in eligible protocols.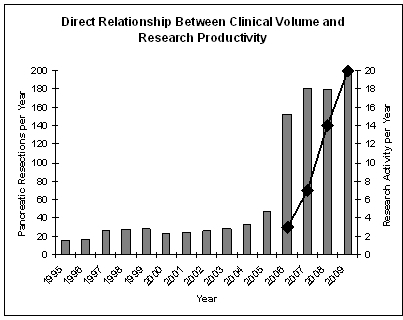
Back to 2011 Program