ADJUVANT THERAPIES FOR R0 RESECTED PN0 STAGE I-III EXTRAHEPATIC CHOLANGIOCARCINOMA: A NATIONAL PERSPECTIVE
Gabriela Aitken1, Andrew M. Fleming1, Paxton V Dickson11. Surgery, The University of Tennessee Health Science Center, Memphis, TN, United States.
Background
The optimal implementation of adjuvant therapy for patients with R0 resected pN0 stage I-III extrahepatic cholangiocarcinoma (eCCA) is not well defined. Current guidelines include options for postoperative observation, adjuvant chemotherapy (CT), or adjuvant chemoradiation (CRT). The current analysis investigates the impact of CT and CRT on overall survival (OS) for these patients.
Methods
Patients with R0 resected pN0 stage I-III eCCA (T1-4N0M0) were identified within the National Cancer Database 2022 "Other Biliary" dataset. Both perihilar and distal eCCA were included. Multiple logistic regressions with odds ratios (OR) and 95% confidence intervals (CI) were used to identify factors associated with receipt of CT and CRT. Kaplan-Meier analysis and multivariable Cox regressions with hazard ratios (HR) and 95% CI assessed the impact of CT and CRT on OS and mortality, respectively.
Results
Among 841 patients included for analysis, 452 underwent resection alone (53.7%), 179 had resection+CT (21.3%), and 210 had resection+CRT (25.0%). Compared to patients who received CT or CRT, those who underwent resection alone were older (69.5 years vs. 67.0 years vs. 63.0 years; P<.0001), more often had 1 or more comorbid conditions (29.0% vs. 15.1% vs. 24.3%; P=.0013), and were less likely to hold private insurance (29.4% vs. 36.3% vs. 51.9%; P<.0001). There were no differences in distribution of perihilar versus distal eCCA between the treatment groups. On multiple logistic regression, receipt of CT was inversely associated with patient age (OR 0.955 per year; CI 0.919-0.991; P=.0173) and comorbid disease (OR 0.356; CI 0.143 - 0.794; P=.0169), and positively associated with stage II disease (OR 3.29; CI 1.133 - 12.19; P=.0446). Receipt of CRT was also associated with stage II disease (OR 5.385; CI 1.982 - 19.05; P=.0028). For patients with stage I disease, there was no significant difference in OS with the addition of CT (logrank P=.0586) or CRT (logrank P=.2128) to R0 resection on time-to-event analysis (Figure 1A). For stage II disease, resection+CT (logrank P=.0026) and resection+CRT (logrank P=.0001) were associated with significantly improved OS compared to resection alone (Figure 1B). Similarly for stage III disease, resection+CT (logrank P=.0057) and resection+CRT (logrank P=.0309) were associated with significantly improved OS compared to resection alone (Figure 1C). On multivariable Cox proportional hazards regression adjusting for age, sex, race, comorbidity, disease stage, grade, and tumor location (perihilar versus distal), both CT (HR 0.561; CI 0.406 - 0.761; P=.0003) and CRT (HR 0.716; CI 0.528 - 0.960; P=.0285) were associated with decreased hazard of death.
Conclusions
In this retrospective analysis, CT and CRT were associated with improved OS for patients with R0 resected pN0 stage II-III perihilar and distal eCCA following R0 resection.
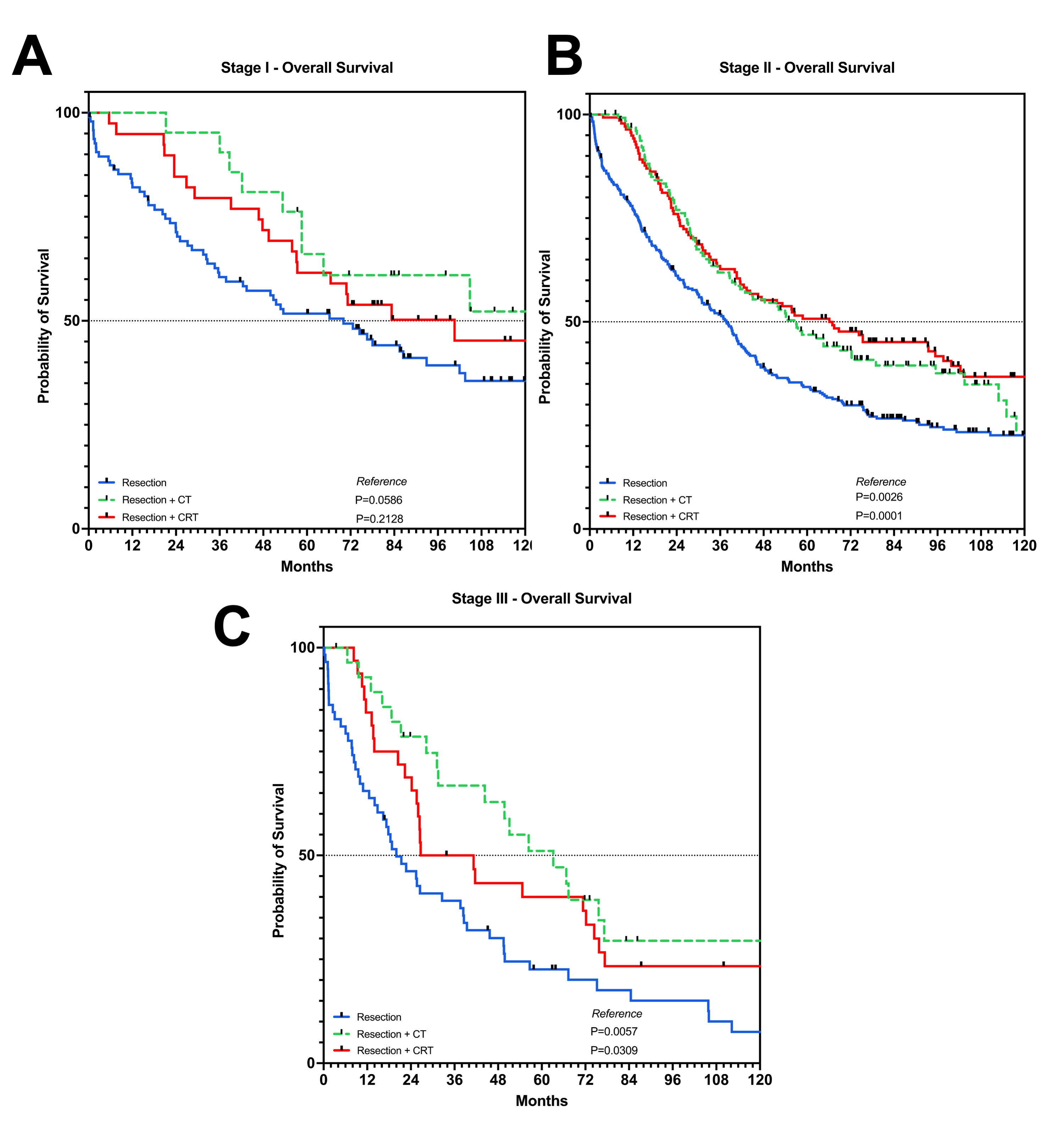 Figure 1. Kaplan Meier curves depicting overall survival for patients with R0 resected N0 (A) stage I, (B) stage II, and (C) stage III extrahepatic cholangiocarcinoma stratified by treatment group. "CT" = chemotherapy. "CRT" = chemoradiation.
Figure 1. Kaplan Meier curves depicting overall survival for patients with R0 resected N0 (A) stage I, (B) stage II, and (C) stage III extrahepatic cholangiocarcinoma stratified by treatment group. "CT" = chemotherapy. "CRT" = chemoradiation.IMAGE CAPTION: Figure 1. Kaplan Meier curves depicting overall survival for patients with R0 resected N0 (A) stage I, (B) stage II, and (C) stage III extrahepatic cholangiocarcinoma stratified by treatment group. "CT" = chemotherapy. "CRT" = chemoradiation.
Back to 2026 Abstracts