TUBE-IN-TUBE ENDOSCOPIC VACUUM THERAPY (TT-EVT) FOR ESOPHAGOJEJUNAL ANASTOMOTIC LEAKS IN ONCOLOGIC PATIENTS
Marcelo Simas de Lima1, Ylanna Fortes Fonseca1, Gustavo Andrade De Paulo1, Renata Nobre Moura1, Bruno da Costa Martins1, Luciano Lenz1, Fernanda Carvalho Franco1, Adriana Medeiros Lima1, Marcelo Morganti Ferreira Dias1, Megui Marilia Mansilla Gallegos1, Caterina Maria Pia Simoni Pennacchi1, Carla Cristina Gusmon Oliveira1, Sebastian Naschold Geiger1, Amanda Aquino de Miranda Pombo1, Marina Tucci Gammaro Baldavira Ferreira1, Andressa Abnader Machado1, Cesar Capel de Clemente1, Adriana Safatle-Ribeiro1, Fauze Maluf Filho11. Endoscopy, Cancer Institute of the State of São Paulo, São Paulo, São Paulo, Brazil.
Introduction: Anastomotic dehiscences are serious postoperative complications after total gastrectomies, with associated mortality rates as high as 25%. Endoscopic vacuum therapy (EVT) has demonstrated its efficacy. TT-EVT is still under evaluation, although its initial results were comparable to classic EVT outcomes for all-cause vacuum therapy, showing technical and clinical success rates of 100% and 86.7%, respectively. This is the first report of this technique in this specific subset of upper GI patients.
Aims: Evaluate technical and clinical successes rates of TT-EVT in the management of esophagojejunal anastomotic leaks and adverse events.
Methods: Retrospective, descriptive analysis of clinical, laboratory, and imaging data from patients treated for esophagojejunal anastomotic leaks with TT-EVT at oncologic referral centers in São Paulo, Brazil.
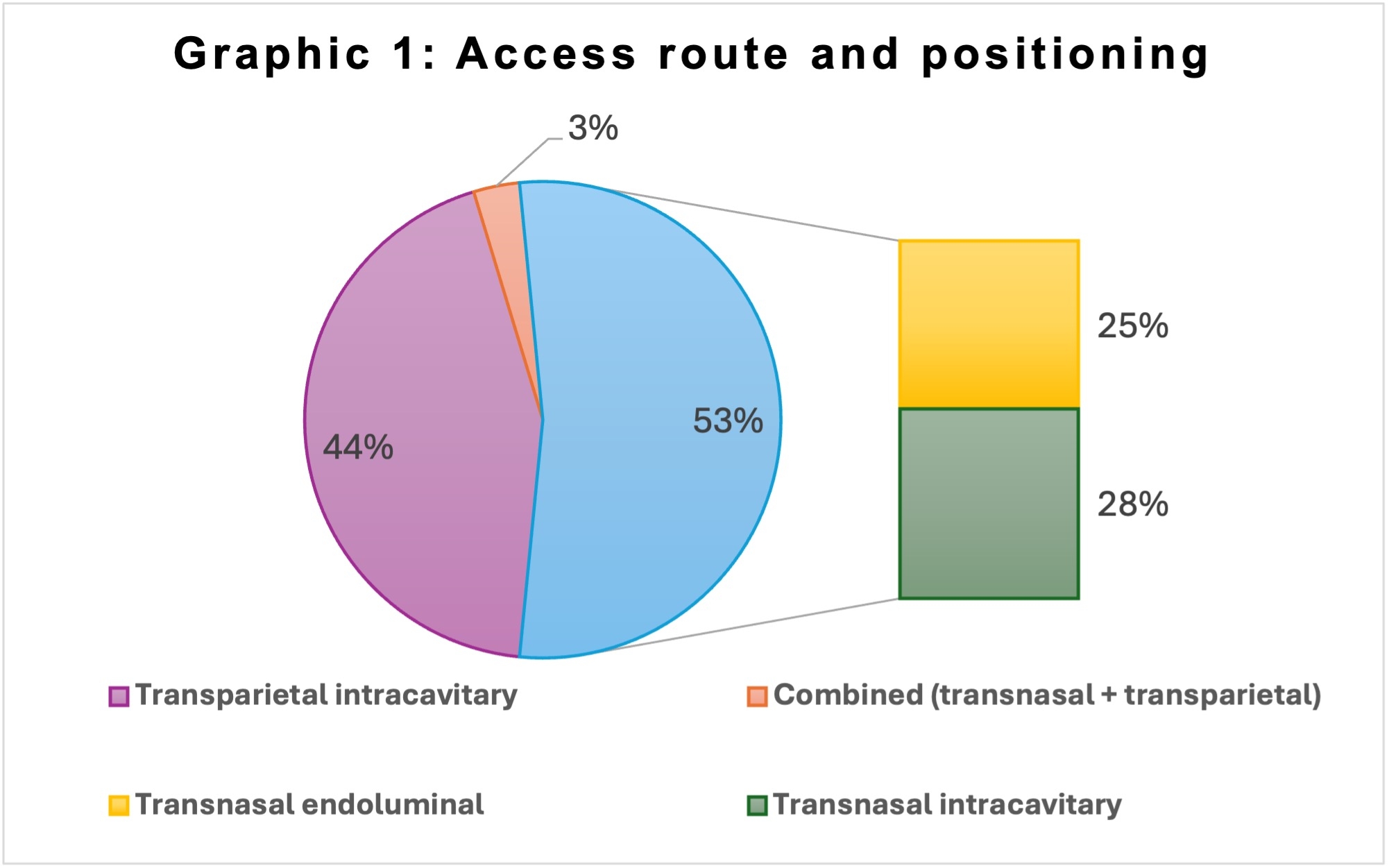
Results: A total of 32 patients with gastric cancer were included. The mean age was 63 years, and 53.1% were male. Twenty-eight patients (87.5%) underwent primary total gastrectomies, while four underwent completion gastrectomies. The mean time between surgery and leak identification was 7 (±3) days. Most leaks were larger than 10 mm (Table 1) and were in the abdomen. TT-EVT was the primary therapy in 24 cases (75%), while in 8 cases it was used as rescue therapy after failure of another treatment. TT-EVT was positioned transnasally in 53.1% of patients, 8 of which on intraluminal position (47.1%) and 9 intracavitary (52.9%). All parietal positioning were intracavitary (43,8%). A combined parietal intracavitary and nasal intraluminal approach was used in one case (3.1%) (Graphic 1). Most patients (70%) were maintained on enteral nutrition. A reduction in C-reactive protein (CRP) levels was observed over the first week, from 186.6 mg/L (±114.4) to 9.64 mg/L (±65.77). An average of 2.8 (±1.7) endoscopies per patient was required, and mean therapy duration was 22 (±14) days. Technical and clinical success rates were 100% and 90%, respectively. Three patients developed stenosis; one required surgery due to an internal hernia. One patient experienced bleeding from the splenic artery. Three patients died.
Conclusions: This study suggests that TT-EVT is an effective treatment for esophagojejunal anastomotic leaks in oncologic patients, demonstrating high technical and clinical success rates. CRP reduction may serve as a valuable marker of early effectiveness in infection control during the first week.

Back to 2026 Abstracts