EARLY SURGERY VS SERIAL ENDOSCOPIC BALLOON DILATION FOR ILEAL CROHN'S STRICTURES: A 15-YEAR MULTICENTER REAL-WORLD COMPARATIVE EFFECTIVENESS STUDY
Ahmed Salem2, Shrouq Khazaaleh1, Asad ur Rahman3, Fatima Khan2, Effa Zahid3, Inas Fouad Soliman Mikhail5, Jana G Hashash4, Mohammad Alomari11. Gastroenterology and Hepatology, University of Arkansas for Medical Sciences, Little Rock, AR, United States.
2. Maimonides Medical Center, New York, NY, United States.
3. Cleveland Clinic Florida, Weston, FL, United States.
4. Mayo Clinic in Florida, Jacksonville, FL, United States.
5. Staten Island University Hospital, New York, NY, United States.
Background and Aims
Endoscopic balloon dilation (EBD) is widely used as a bowel-preserving strategy for ileal Crohn's disease strictures, but recurrence and progression to surgery remain common. Whether early surgical resection provides superior long-term outcomes versus serial dilation is unclear. We compared outcomes after early ileal resection with serial EBD in patients with isolated nonpenetrating ileal strictures.
Methods
Using the TriNetX Global Network (2010-2025), we identified adults with newly diagnosed ileal Crohn's disease and imaging-confirmed strictures within six months. Patients with prior bowel surgery, penetrating or perianal disease, abscess, or fistula were excluded. Management within six months defined cohorts as early resection or serial EBD (≥2 dilations within 12 months). Propensity-score matching (1:1) balanced baseline inflammatory markers, stricture features, corticosteroid exposure, biologic initiation, and demographics. The primary outcome was subsequent bowel surgery beyond six months. Secondary outcomes included obstruction hospitalization, new abscess, steroid exposure beyond three months, biologic initiation, and endoscopic complications within two years. Kaplan-Meier and Cox models estimated adjusted hazard ratios (aHR).
Results
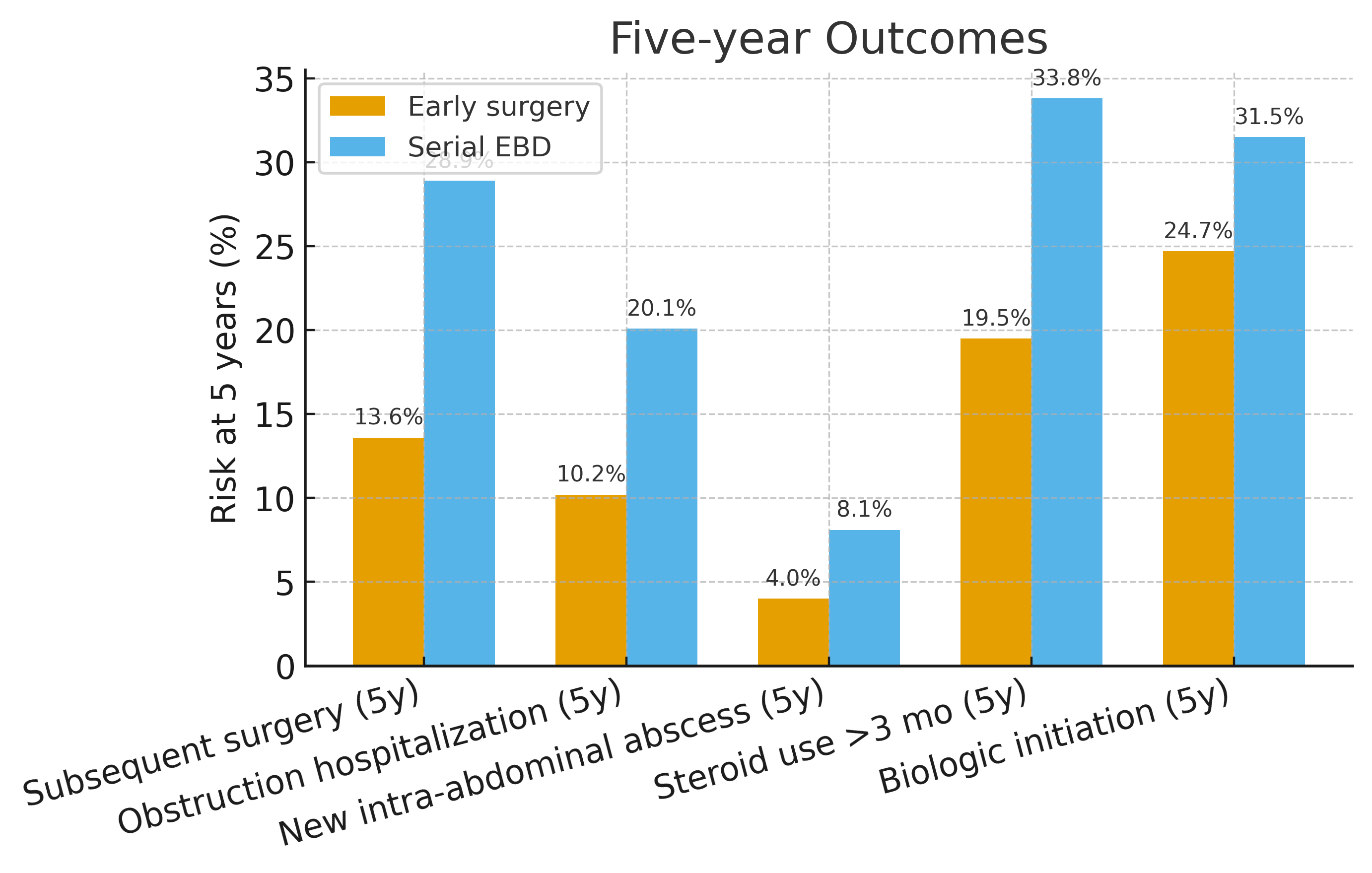
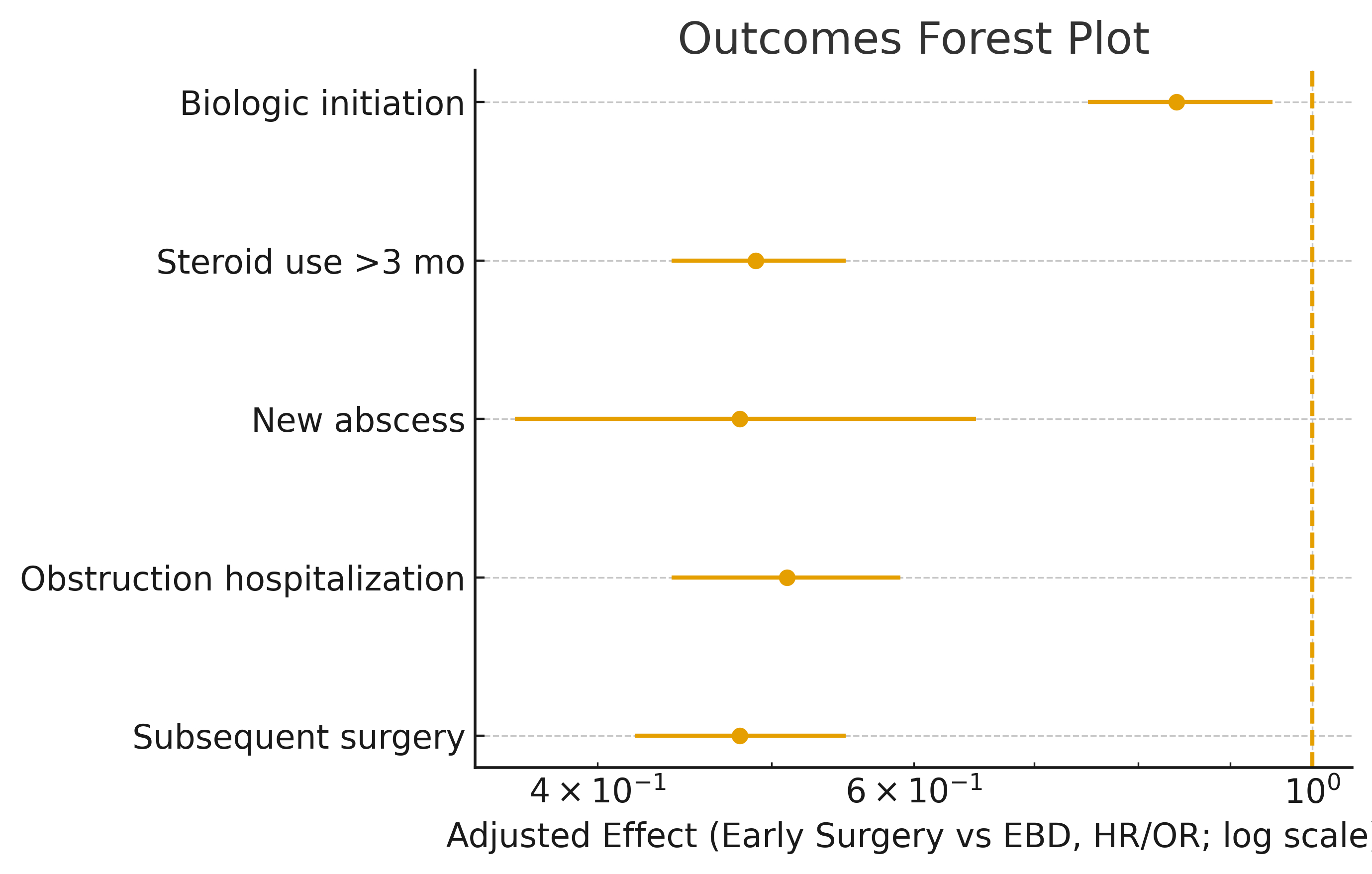
After matching, 3,842 patients were included per group. Early surgery significantly reduced subsequent surgery compared with EBD (7.8% vs 15.9%; aHR 0.48; 95% CI 0.42-0.55). Obstruction hospitalization was lower after surgery (5.8% vs 11.6%; aHR 0.51; 95% CI 0.44-0.59). New abscess developed in 1.7% versus 3.5%, and prolonged steroid exposure occurred in 10.7% versus 20.3%. Biologic initiation was slightly reduced in the surgery group. Perforation or bleeding occurred in 0.76% with EBD, with none after early surgery. Two-year surgery-free survival favored resection (91.9% vs 81.1%). Findings were consistent across stricture length, inflammatory burden, and smoking status; sensitivity analyses requiring ≥3 dilations showed similar results.
Conclusions
Early ileal resection within six months was associated with lower risks of reoperation, obstruction, abscess, steroid dependence, and procedural complications compared with serial dilation. These data support considering early surgery for selected nonpenetrating ileal strictures and reinforce the importance of interdisciplinary treatment planning.
Back to 2026 Abstracts