VENTRAL HERNIA COMPLEXITY DOES NOT PREDICT FUNCTIONAL OUTCOMES: OBJECTIVE PERFORMANCE AND QUALITY OF LIFE FINDINGS FROM ABVENTURE-P
Sidhant Kalsotra2, Mengda Yu3, Kiana Shannon2, Peter Edwards2, Savannah Renshaw2, Elanna Arhos1, Lai Wei3, Stephanie Di Stasi4, 5, Ajit Chaudhari5, 6, 7, Benjamin Poulose21. Department of Physical Therapy and Human Movement Sciences, Northwestern University, Evanston, IL, United States.
2. The Ohio State University Department of Surgery, Columbus, OH, United States.
3. Department of Biomedical Informatics, Center for Biostatistics, Ohio State University Wexner Medical Center, Columbus, OH, United States.
4. The Ohio State University Division of Physical Therapy, Columbus, OH, United States.
5. The Ohio State University Wexner Medical Center Sports Medicine Research Institute, Columbus, OH, United States.
6. The Ohio State University School of Health and Rehabilitation Sciences, Columbus, OH, United States.
7. Department of Biomedical Engineering, The Ohio State University, Columbus, OH, United States.
Introduction: Predicting functional outcomes after ventral hernia repair remains challenging. We investigated whether hernia complexity, assessed using the modified Ventral Hernia Working Group (VHWG) classification, predicts functional outcomes at 1-year using objective performance measures and patient-reported quality of life.
Methods: We conduceted a secondary analysis of the ABVENTURE-P randomized trial (NCT05142618) partial data between April 2022-August 2024. Participants were stratified at baseline using modified VHWG into Lower Complexity (Grade 1, n=41) and Higher Complexity (Grades 2-3 combined, n=67) groups. Of 108 participants with baseline data, 53 (49.1%) had completed 1-year assessments by March 2025 including, objective performance (Five Times Sit-to-Stand [5xSTS], Timed Up and Go [TUG]) and patient-reported outcomes (Hernia-Related Quality of Life Survey (HerQLes); higher scores = better QoL, 0-100 scale). Generalized linear models assessed 1-year outcomes adjusting for baseline functional performance, BMI, age, sex, race, ethnicity.
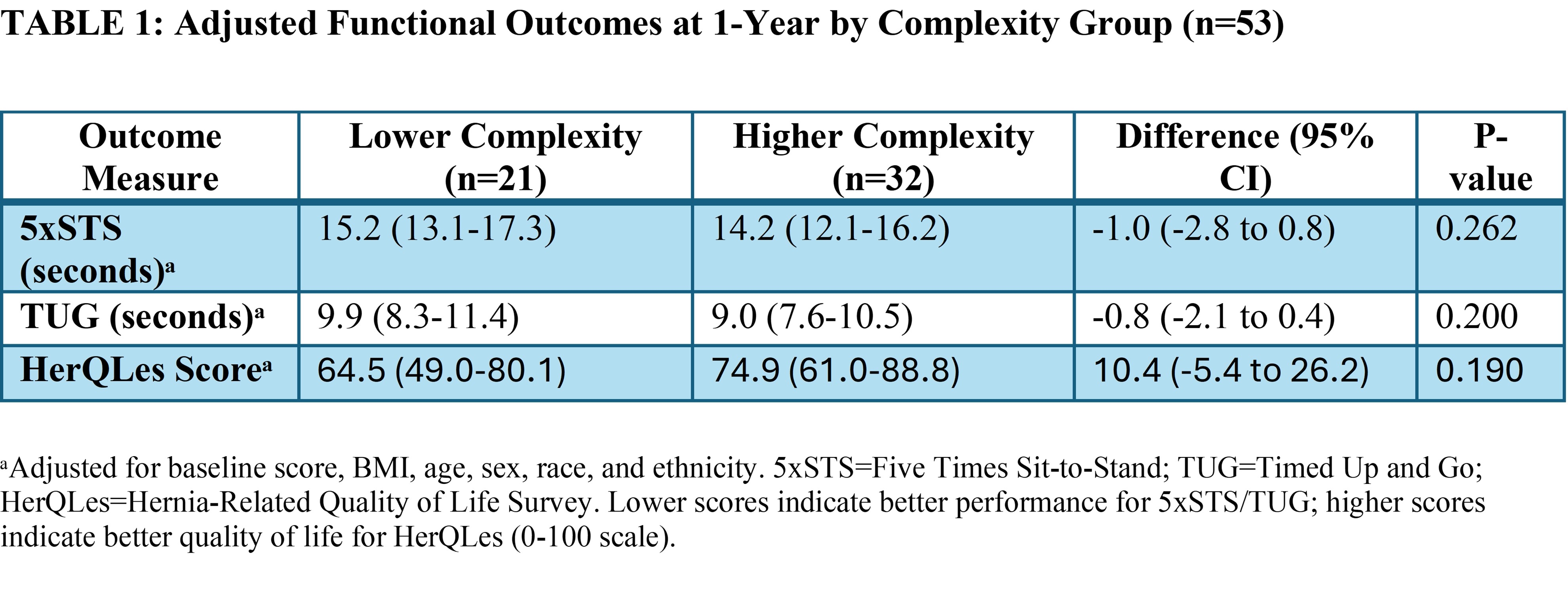
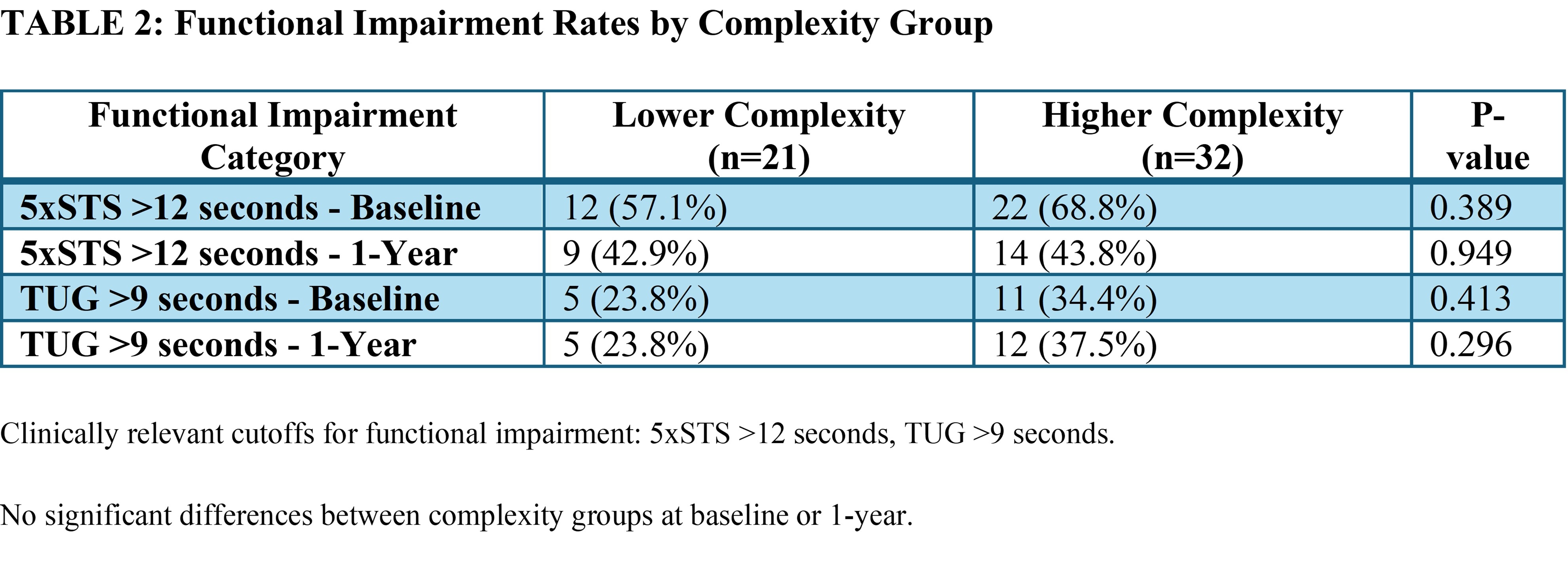
Results: The cohort included 21 Lower Complexity patients (mean age 52.3 years, BMI 30.1, 42.9% female) and 32 Higher Complexity patients (mean age 48.7 years, BMI 35.1, 40.6% female). At 1-year post-operatively, functional outcomes did not differ by complexity group across all measures (Table 1). Adjusted mean 5xSTS times were 15.2 seconds (Lower) vs 14.2 seconds (Higher), p=0.262. Adjusted mean TUG times were 9.9 vs 9.0 seconds, p=0.200. Adjusted mean HerQLes scores showed no difference between groups (64.5 vs 74.9, p=0.190), with both groups demonstrated improvement in HerQLes scores from baseline to 1-year (Lower: from 49.2 to 72.4, +23.1 points; Higher: from 41.2 to 74.8, +33.6 points), with no significant difference in 1-year adjusted scores (p=0.190). When categorized using clinically relevant cutoffs, similar proportions of patients in both complexity groups showed functional impairment at baseline and 1-year (Table 2).
Conclusion: In this secondary analysis of ABVENTURE-P trial participants, functional performance and patient-reported outcomes at 1-year post-VHR did not differ by hernia complexity. Participants with higher complexity hernias achieved comparable outcomes to lower complexity patients despite greater comorbidity burden. However, caution is warranted in generalizing these findings, as this was an exploratory secondary analysis not specifically powered to detect differences between complexity groups, and only 49% of participants had completed 1-year assessments at the time of analysis. These preliminary findings suggest that surgeons should exercise caution in using complexity grades to set patient expectations for functional outcomes. Future research should develop function-specific risk stratification tools incorporating baseline functional status and patient-centered goals.
Back to 2026 Abstracts