TIME-DEPENDENT RECURRENCE RISK AND PROGNOSTIC FACTORS AFTER HEPATIC RESECTION FOR NEUROENDOCRINE LIVER METASTASES
Kyoji Ito1, Mikel Madi1, Yoshikuni Kawaguchi2, Elena Panettieri3, Adriana C. Gamboa1, Timothy E Newhook1, Yun Shin Chun1, Hop S Tran Cao1, Ching-Wei D Tzeng1, Jean-Nicolas Vauthey1, Jessica E. Maxwell11. Surgical Oncology, MD Anderson Cancer Center, Houston, TX, United States.
2. Tokyo Daigaku, Bunkyo, Tokyo, Japan.
3. Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Lazio, Italy.
Background: Neuroendocrine liver metastases (NELM) frequently recur after hepatic resection; however, the temporal dynamics of recurrence risk remain poorly understood. We sought to identify time-dependent recurrence risk and prognostic factors to allow us to optimize our postoperative surveillance strategy.
Methods: In this international multicenter study, 329 patients who underwent initial complete treatment by hepatic resection with or without ablation for NELM during 1995-2004 at three hepatobiliary centers were analyzed. Recurrence-free survival and overall survival were estimated using Kaplan-Meier methods. Time-varying risks of recurrence and death were assessed with kernel-smoothed hazard estimates. Prognostic factors were evaluated using univariable and multivariable Cox regression analyses.
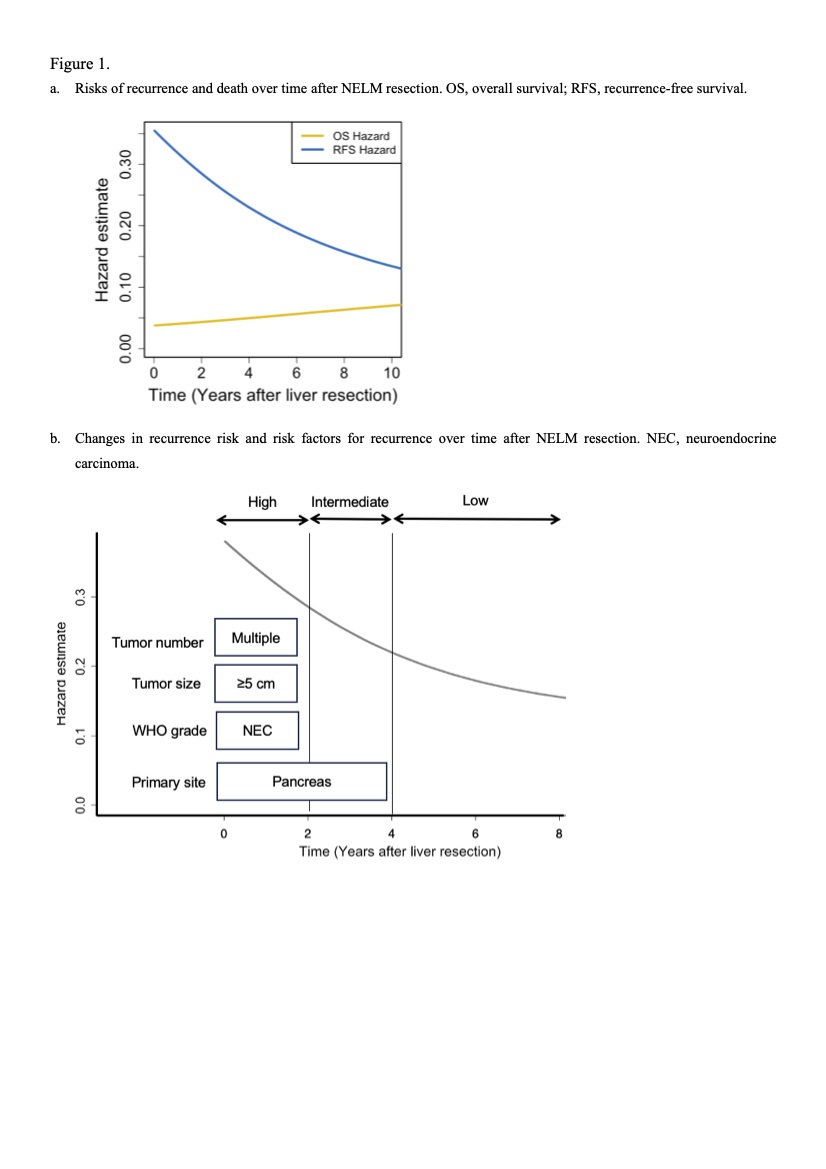
Results: The risk of recurrence was highest immediately after surgery and declined over time yet did not reach zero 10 years after resection (Figure 1a). Multivariable analysis identified pancreatic primary tumor (hazard ratio [HR] 1.92), multiple liver metastases (HR 1.80), maximum liver tumor diameter >5 cm (HR 1.64), and neuroendocrine carcinoma (HR 2.57) as independent predictors of recurrence (Table 1). Conditional analysis demonstrated that beyond 2 years of recurrence-free survival, only pancreatic primary tumor remained a significant risk factor (Table 1). Based on time-dependent prognostic factors, we propose a risk-adapted surveillance strategy (Figure 1b): Patients with pancreatic primary tumors should undergo imaging every 3-4 months during the first 4 years and then transition to imaging every 6-12 months, with follow-up extending beyond 10 years. Patients with multiple metastases, maximum tumor diameter >5 cm, or neuroendocrine carcinoma should undergo imaging every 3-4 months during the first 2 years and then transition to imaging every 6-12 months, with follow-up extending beyond 10 years.
Conclusions: The risk of recurrence and the prognostic factors for recurrence after NELM resection change over time. A tailored surveillance approach may meaningfully reduce unnecessary imaging, radiation exposure, and travel burden for lower-risk patients while improving the likelihood of timely detection and intervention in patients at higher risk.

Back to 2026 Abstracts