REGIONAL NODAL STATUS INFLUENCES RECURRENCE PATTERNS FOLLOWING HEPATECTOMY FOR MULTIFOCAL INTRAHEPATIC CHOLANGIOCARCINOMA
Kever A. Lewis1, Elena Panettieri2, Galen Gist1, Francesco Ardito2, Mario De Bellis3, Andrea Ruzzenente3, Iolanda Scoleri4, Emmanueal Boleslawski4, Kristoffer W. Brudvik5, Flavio Milana6, Guido Torzilli6, Guillauma Passot7, Madhulika Eluri1, Sunyoung S. Lee1, Z. Ian Hu1, Shubham Pant1, Milind Javle1, Adriana C. Gamboa1, Yun Shin Chun1, Ching-Wei D Tzeng1, Felice Giuliante2, Jean-Nicolas Vauthey1, Hop S Tran Cao1, Timothy E Newhook11. The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
2. Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Lazio, Italy.
3. Azienda Ospedaliera Universitaria Integrata Verona Sede di Borgo Roma, Verona, Veneto, Italy.
4. Centre Hospitalier Universitaire de Lille, Lille, Hauts-de-France, France.
5. Oslo universitetssykehus, Oslo, Oslo, Norway.
6. IRCCS Humanitas Research Hospital, Rozzano, Lombardia, Italy.
7. Hospices Civils de Lyon, Lyon, Auvergne-Rhône-Alpes , France.
Recurrence after hepatectomy for intrahepatic cholangiocarcinoma (iCCA) is common, and patients with multifocal or node-positive tumors are at highest risk. Unfortunately, recurrences are often unsalvageable and not amenable to local therapies in this high-risk population. We sought to evaluate recurrence patterns following hepatectomy in a large, international cohort to inform salvage strategies after hepatectomy.
Patients undergoing curative-intent hepatectomy for iCCA from January 2000 to August 2024 were identified from an international consortium of 7 high-volume hepatobiliary centers. Recurrences were classified as liver only (LO) or systemic (SYS). Rates of recurrence were modeled with cumulative incidence functions using Gray comparisons.
Among 615 resected patients (median follow-up 67.6 months), 25% (n=157) of patients underwent hepatectomy for multifocal disease of which 44% (69/157) had regional nodal metastases (pN1). Preoperative chemotherapy was given to 22%, and 52% received postoperative chemotherapy. Overall recurrence rate was 69% (n=427) at a median of 15.3 months following hepatectomy. Patients with multifocal tumors had a shorter recurrence-free survival compared to those with solitary tumors (median, 8.3 months vs. 21.4 months; p<0.001). Over the study period, 14% (n=21) of patients with multifocal disease remained recurrence-free compared to 39% of patients with solitary disease. Within 3 years, patients with multifocal disease had more LO (41% vs 25%, p<0.001) and SYS recurrences (45% vs 36%, p=0.009). For those patients with SYS recurrences, multifocal tumors had higher rates of lung (29%) and bone (19%) metastases whereas solitary tumors more often recurred in lymph nodes (24%). Among patients with multifocal tumors, pN1 disease resulted in higher cumulative rates of recurrence compared to pN0 (94% vs 80%). Having multifocal pN1 iCCA was associated with higher incidence of SYS recurrences at 1- and 2- years (51% vs. 21% at 1 year; 60% vs 31% at 2 years, p< 0.001; Fig. 1a). Rates of LO recurrence for patients with multifocal disease did not differ based on nodal classification (p=0.203; Figure 1b). All recurrences in patients with multifocal pN1 tumors occurred within 3 years of hepatectomy. After recurrence, patients with multifocal disease had a median overall survival (OS) of 24.9 months after LO recurrence and 14.3 months after SYS recurrence (p=0.350; Fig. 2). However, patients with multifocal disease demonstrated a higher 1- and 2-year OS following LO recurrence compared to SYS recurrences (76% vs 56% at 1 year; 53% vs. 35% at 2 years).
Following hepatectomy for iCCA, multifocal disease results in earlier and higher rates of LO and SYS recurrence. However, patients with resected multifocal but pN0 disease have less systemic recurrences and thus may benefit from recurrence-directed local and regional salvage therapies.
 Figure 1. Cumulative incidence of (a) liver only and (b) systemic recurrence in patients with multifocal iCCA based on nodal status
Figure 1. Cumulative incidence of (a) liver only and (b) systemic recurrence in patients with multifocal iCCA based on nodal status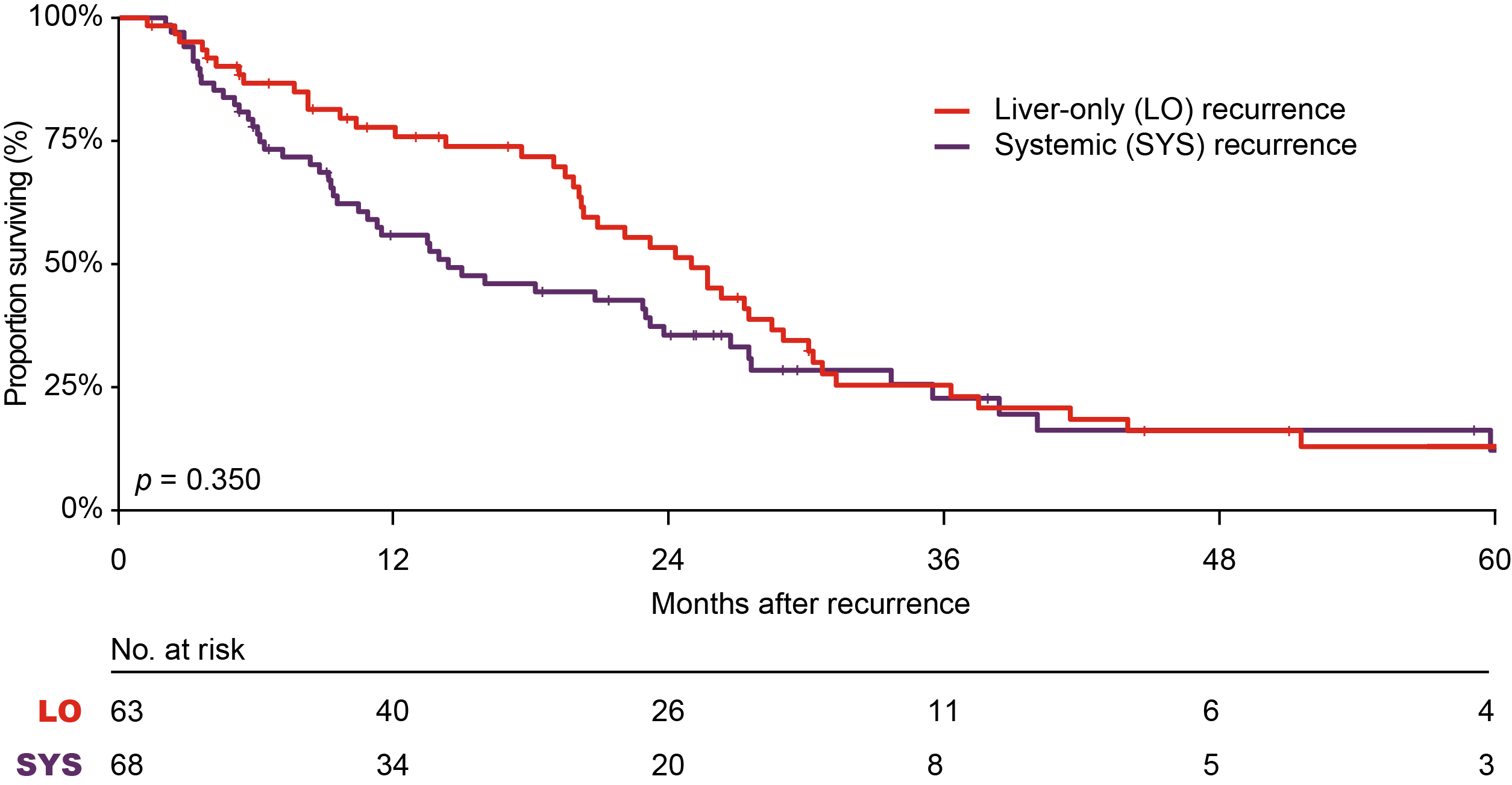 Figure 2. Overall survival following recurrence based on site of initial recurrence. LO, liver only recurrence. SYS, systemic recurrence.
Figure 2. Overall survival following recurrence based on site of initial recurrence. LO, liver only recurrence. SYS, systemic recurrence.IMAGE CAPTION: Figure 1. Cumulative incidence of (a) liver only and (b) systemic recurrence in patients with multifocal iCCA based on nodal status
Figure 2. Overall survival following recurrence based on site of initial recurrence. LO, liver only recurrence. SYS, systemic recurrence.
Back to 2026 Abstracts