DOES TYPE OF FUNDOPLICATION AFFECT RECURRENCE RATES FOLLOWING PARAESOPHAGEAL HERNIA REPAIR?
Ayesha Siddiq1, 2, Nicholas Catanzaro2, Mujjahid Abbas1, 2, Joshua Lyons1, 2, Hamza Chatha1, 2, Patrick Wieland1, 2, Saher-Zahra Khan1, 2, Nicolette M Winder1, 2, Samuel J Zolin1, 2, Jeffrey M. Marks1, 2, Leena Khaitan1, 21. Surgery, University Hospitals Health System, Cleveland, OH, United States.
2. Case Western Reserve University, Cleveland, OH, United States.
Background:
Fundoplication is frequently used during paraesophageal hernia (PEH) repair to enhance reflux control and reduce recurrence. Prior institutional data showed that adding a fundoplication to PEH repair increased hernia recurrence (19% vs 12%) without reducing the need for reoperation. We aim to evaluate the influence of fundoplication type on postoperative recurrence of PEH.
Methods:
Utilizing our institutional database, demographic, operative and follow up data collected for those having elective minimally invasive (MIS) PEH repair with fundoplication (2016-2023). Exclusion criteria: No documented fundoplication type or had concomitant procedures. The primary outcome was documented radiographic or endoscopic hernia recurrence postoperatively. Secondary outcomes included symptom recurrence, and reoperation. Fundoplication type was primary exposure.
Univariable analyses were performed using chi-square and t-tests, and multivariable logistic regression evaluated independent associations between fundoplication type and recurrence.
Results:
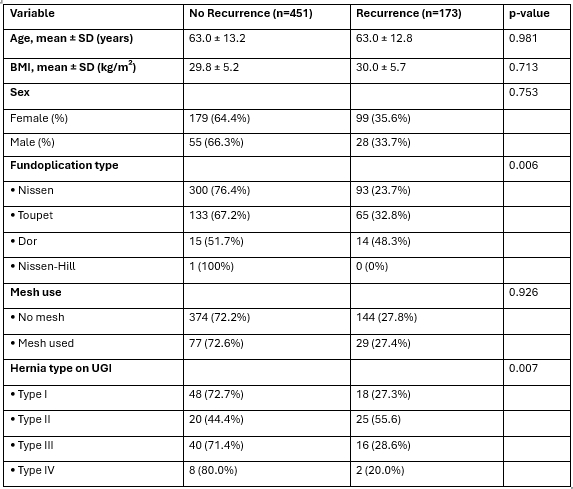
Analysis identified 624 adults with mean age 62.9 ± 13.1 years and mean BMI 29.9 ± 5.3 kg/m2. Post-operative recurrence occurred in 27.7% of patients at latest follow up. Recurrence rates differed significantly by fundoplication technique, with Nissen (NF) demonstrating the lowest recurrence rate (23.66%), followed by Toupet (TF) (32.83%) and Dor (DF) (48.28%) (p = 0.006).
Mesh and non-mesh groups had similar recurrence rates with NF (24.0% vs 23.6%) and TF repairs (29.4% vs 34.0%). DF repairs had highest recurrence regardless of mesh use (40.0% vs 50.0%). Symptom recurrence noted with dysphagia (32%), reflux/heartburn (39%), nausea and emesis (15% each), and chest pain (13%). Symptom patterns were similar across all wrap types. Overall, 27 patients (16%) were completely asymptomatic.
41 patients (23.8%) underwent reoperation with no statistically significant association with fundoplication type (NF 27.9%, TF 16.9%, DF 28.6%; p = 0.25). Median time to reoperation was 14.5 months (IQR 2.0-31.2) and differed across fundoplication types [(NF: 16.9 months (IQR 4.1-42.8), TF: 7.1 months (IQR 0.07-22.4), DF: 10.5 months (IQR 1.2-25.0)].
Primary multivariable analysis adjusting for age and BMI, both TF (OR 1.59, 95% CI 1.09-2.33; p = 0.016) and DF (OR 3.06, 95% CI 1.41-6.61; p = 0.005) were independently associated with higher odds of postoperative recurrence compared with NF, while age and BMI were not predictive.
Conclusion:
Recurrence rates were higher than our earlier institutional data, likely reflecting the expanded dataset. NF had the lowest recurrence risk, TF and DF had significantly higher rates. These findings suggest complete 360-degree wraps offer more protection against recurrence than partial wraps in PEH repair and increase time to recurrence.
Back to 2026 Abstracts