COMPARATIVE RISK OF POSTOPERATIVE GASTROPARESIS AFTER POEM VERSUS HELLER MYOTOMY FOR ACHALASIA
Ahmed Aly1, 2, Penelope Rechtorovic1, 2, Vineeth Sadda1, 2, Himsikhar Khataniar2, 4, Ping Zheng1, 2, Shahin Ayazi1, 2, 31. Foregut Division, Surgical Institute, Allegheny Health Network, Pittsburgh, PA, United States.
2. Chevalier Jackson Esophageal Research Center, Western Pennsylvania Hospital, Allegheny Health Network, Pittsburgh, PA, United States.
3. Department of Surgery, Drexel University, Philadelphia, PA, United States.
4. Department of Medicine, Allegheny Health Network, Pittsburgh, PA, United States.
Introduction:
Achalasia is a primary esophageal motility disorder often treated with Heller myotomy with partial fundoplication (HM) or peroral endoscopic myotomy (POEM). Both procedures relieve esophageal outflow obstruction, but their effects on gastric motility are less well defined. Some achalasia patients develop gastroparesis as part of their disease course, raising the possibility of a broader motility disorder or, with HM, a consequence of surgical dissection and potential vagal disruption. Comparative data on postoperative gastroparesis after HM versus POEM remains limited. This study evaluated the risk of new-onset gastroparesis following these procedures.
Methods:
We queried a large, multi-institutional U.S. electronic health record network to identify adults with achalasia who underwent HM or POEM between 2010 and 2023. Patients with prior foregut surgery, gastroparesis, or prokinetic use were excluded. The primary outcome was new-onset gastroparesis within 2 years. Secondary outcomes included initiation of prokinetics and symptoms suggestive of gastroparesis (nausea, vomiting, bloating, abdominal pain or early satiety). Propensity score matching balanced demographics and comorbidities. Subgroup analyses evaluated patients with diabetes and with GI dysmotility disorders including irritable bowel syndrome, chronic constipation, and small intestinal bacterial overgrowth.
Results:
A total of 4,442 HM and 1,222 POEM patients were identified. After matching, HM had a higher incidence of new gastroparesis (2.09% vs 0.92%, OR 2.28, p=0.019) and greater prokinetic initiation (7.36% vs 4.82%, OR 1.57, p=0.014). Symptoms suggestive of gastroparesis were similar between groups (10.40% vs 9.99%, OR 1.05, p=0.737).
In the HM cohort, diabetics had higher risk of gastroparesis or prokinetic initiation compared with non-diabetics (12.19% vs 8.02%, OR 1.59, p=0.020). In the POEM cohort, this combined endpoint did not differ between diabetics and non-diabetics (8.85% vs 6.40%, OR 1.42, p=0.358) (Figure).
Patients with preexisting GI dysmotility disorders also had increased risk of new gastroparesis after both procedures. This included HM (17.62% vs 6.82%, OR 2.92, p<0.0001) and POEM (13.92% vs 4.79%, OR 3.22, p=0.002). Direct comparison between dysmotility patients undergoing HM versus POEM showed no significant difference (p=0.455) (Figure).
Conclusion:
HM was associated with higher rates of postoperative gastroparesis and prokinetic initiation than POEM, likely reflecting greater procedural effects on vagal pathways and gastric function. Increased risk in diabetics and in patients with GI dysmotility disorders indicates underlying motility susceptibility contributes. These findings suggest postoperative gastric dysfunction reflects both procedure-related and patient-specific factors, supporting individualized procedure selection and counseling in achalasia.
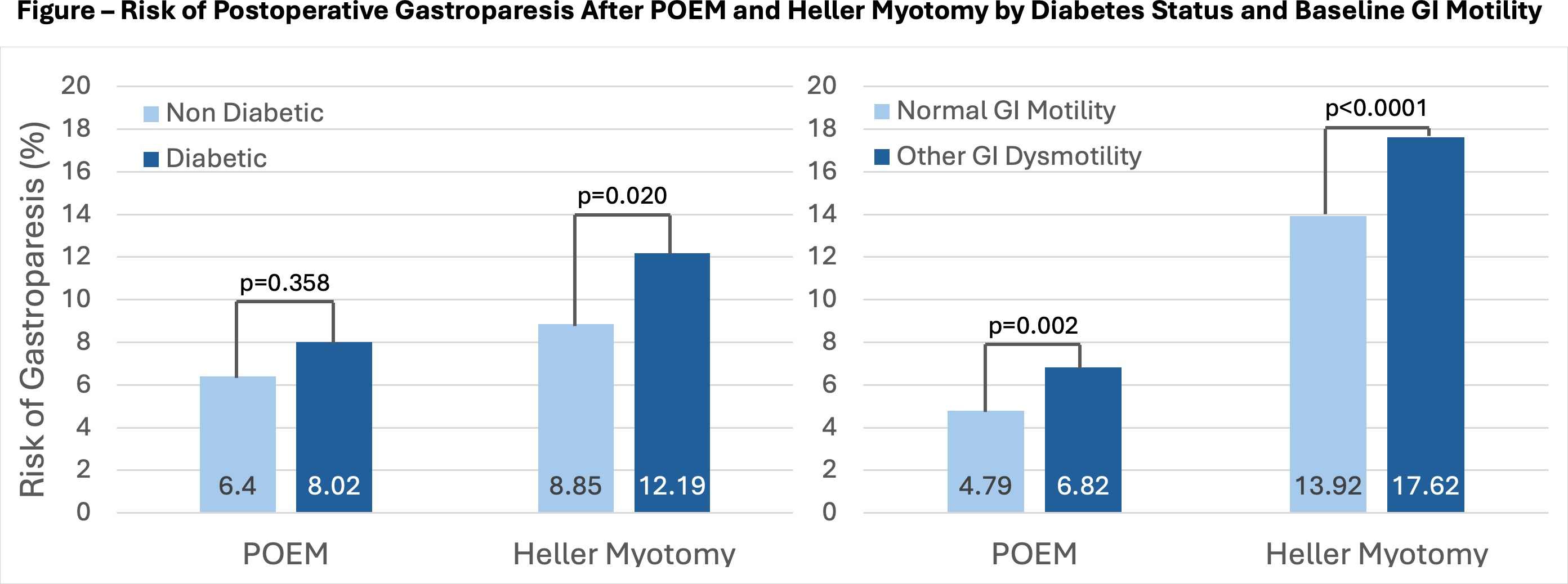 Risk of postoperative gastroparesis after POEM and Heller myotomy by diabetes status and baseline GI motility
Risk of postoperative gastroparesis after POEM and Heller myotomy by diabetes status and baseline GI motilityIMAGE CAPTION: Risk of postoperative gastroparesis after POEM and Heller myotomy by diabetes status and baseline GI motility
Back to 2026 Abstracts