RECURRENCE PATTERNS AND SURVIVAL IN RESECTED T4 COLON ADENOCARCINOMA
Ryan B Morgan1, Kilian Brown1, Taylor Neilson1, Megan Delisle1, Kentaro Ochiai1, Y. Nancy You1, Brian Keith Bednarski1, Tsuyoshi Konishi1, Ramy S Behman1, Jeongyoon Moon1, Craig A Messick1, Montserrat Guraieb Trueba1, Miguel Rodriguez Bigas1, George J Chang1, Josh Smith1, Paul Mansfield1, Yun Song1, Beth Helmink1, Keith Fournier1, Paula Marincola Smith1, Michael White11. Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Introduction: Locally advanced (T4) colon adenocarcinoma is associated with an increased risk of recurrence, particularly to the peritoneum. Here we report the long-term risk of recurrence following curative intent surgery for T4 colon adenocarcinoma.
Methods: A retrospective review of a prospectively maintained database of patients undergoing curative resection for colon adenocarcinoma at a single high-volume referral center was performed (2005-2023). Patients with pathologic T4 disease were included as well as those with clinical T4 disease down-staged following neoadjuvant systemic therapy. Patients with recurrent disease were separated into two groups by site of initial recurrence: those with recurrence limited to the peritoneum (PM) versus those with recurrence outside of the peritoneum (extraperitoneal metastases, EPM). Patients with concurrent peritoneal and extraperitoneal initial recurrences were included in the EPM group. Kaplan-Meier survival analyses were performed to evaluate time to recurrence and overall survival (OS) following recurrence.
Results: Two hundred and sixty-six patients were identified during the study period (median age 63). Primary tumors were most frequently located in the descending or sigmoid colon (53.3%) and were most commonly moderately differentiated (63%). One hundred and sixteen (43.6%) patients had a perforation or obstruction, and most patients had high risk histopathologic features including lymphovascular invasion (66%), tumor deposits (23.3%), or lymph node metastasis (57.5%). Forty-four patients (16.5%) had clinical T4 disease on pre-operative imaging that was downstaged following neoadjuvant therapy. After a median follow up of 5.6 years [IQR 3.9-8.9], the overall recurrence rate was 25.6% (n=68). Two patients with anastomotic recurrence were excluded from subsequent analyses of patients with metastatic disease. Among those who developed metachronous metastases, 29 (43.9%) had isolated PM while 37 (56.1%) had EPM. Six patients in the EPM group had simultaneous peritoneal recurrences. Median time to recurrence was similar between PM and EPM groups (14.3 vs. 12.7 months, p=0.97). Overall survival (OS) after recurrence was similar for both PM and EPM (Median 41.3 vs. 43.9 months, p=0.47). Patients with initially isolated PM underwent re-operation more often than those with EPM (48.3% vs. 27.0%, p=0.12). Within the PM group, median OS after recurrence was longer for patients selected to undergo re-operation compared to those treated non-operatively (63.9 vs 33.2 months, p=0.01) [Figure 1].
Conclusion: Rates of recurrent PM and EPM following curative resection for T4 colon adenocarcinoma are similar, and durable survival is achievable for both cohorts. Re-operation for isolated peritoneal recurrence was associated with long-term survival in well-selected patients.
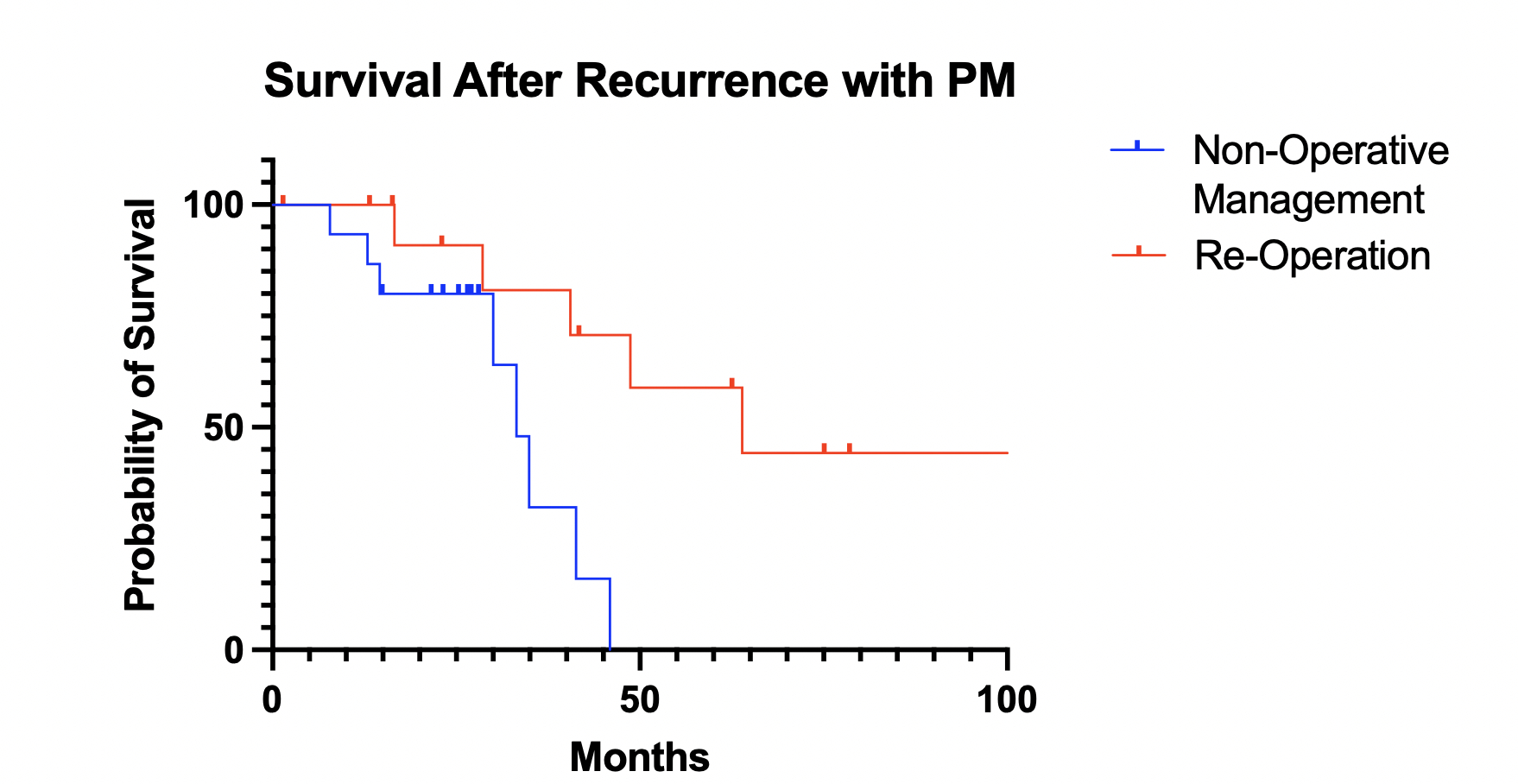 Figure 1: Kaplan-Meier analysis of survival after recurrence for patients with isolated peritoneal metastases undergoing re-operation compared to non-operative management.
Figure 1: Kaplan-Meier analysis of survival after recurrence for patients with isolated peritoneal metastases undergoing re-operation compared to non-operative management.IMAGE CAPTION: Figure 1: Kaplan-Meier analysis of survival after recurrence for patients with isolated peritoneal metastases undergoing re-operation compared to non-operative management.
Back to 2026 Abstracts