AMERICAN JOINT COMMITTEE ON CANCER TUMOR REGRESSION GRADE AFTER NEOADJUVANT THERAPY: IMPLICATIONS FOR LONG-TERM OUTCOMES IN RECTAL CANCER.
Michel Gardere Camargo1, Scott Steele1, Mikhael Belkovsky1, Stefan D. Holubar1, Michael Valente1, Hermann Kessler1, David Liska1, Leonardo Duraes11. Cleveland Clinic, Cleveland, OH, United States.
Introduction The American Joint Committee on Cancer (AJCC) regression grading system is the preferred classification for reporting the pathological response to neoadjuvant therapy in rectal cancer. However, its relationship to long-term oncologic outcomes remains insufficiently defined. We hypothesized that better pathological response is associated with improved oncologic outcomes. This study evaluated the association between AJCC regression grades and long-term outcomes in rectal cancer patients treated at a high-volume referral center.
Methods: We performed a single-center retrospective cohort study of patients with primary rectal adenocarcinoma who underwent neoadjuvant therapy followed by curative-intent surgery between 2000 and 2020 and had a documented AJCC regression grade score. AJCC grades were defined as follows: 0"�no viable tumor cells; 1"�single cells or small clusters; 2"�tumor cells present with predominant fibrosis; 3"�minimal or no tumor response. Demographics, oncologic, and recurrence outcomes were compared among different AJCC grades.
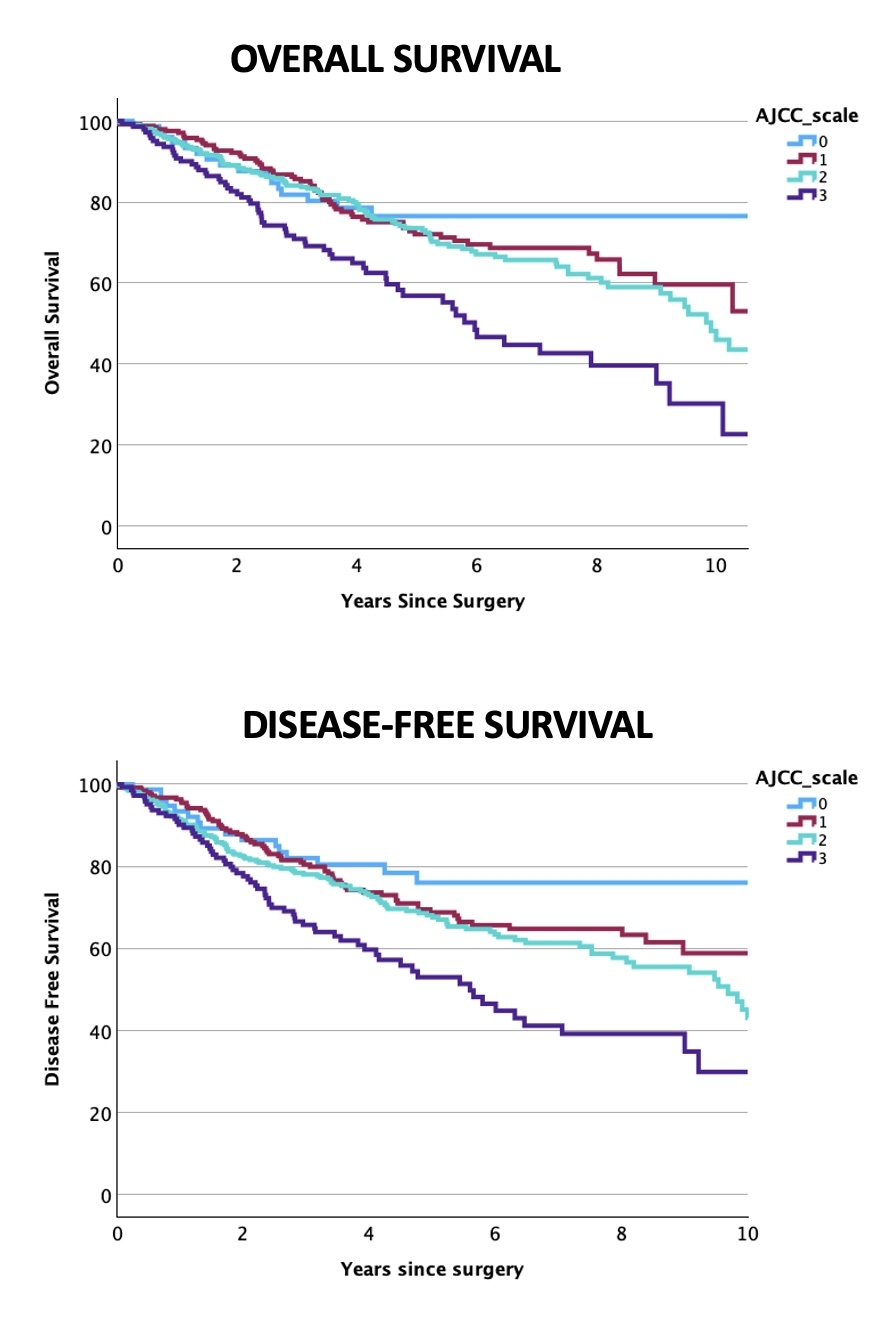
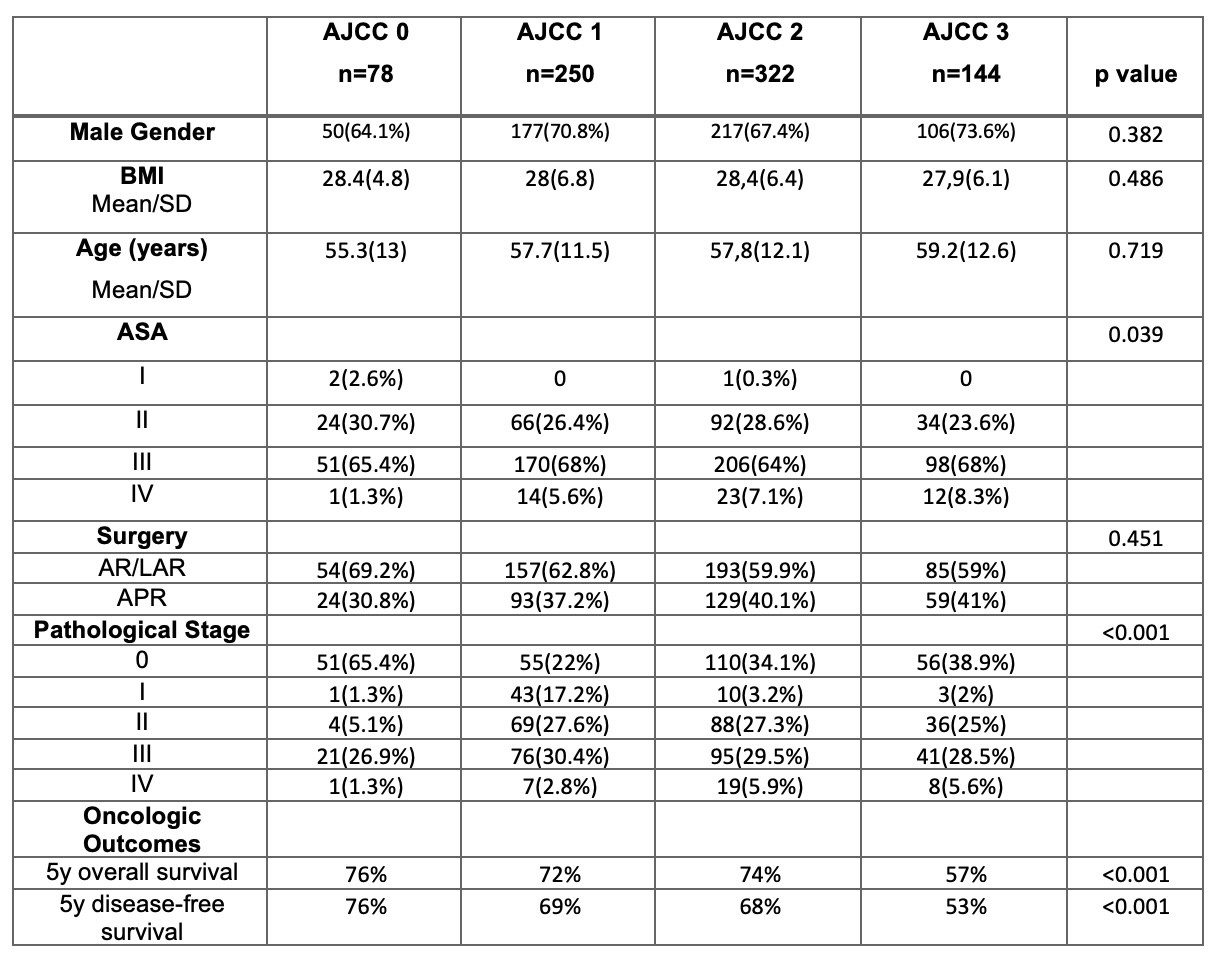
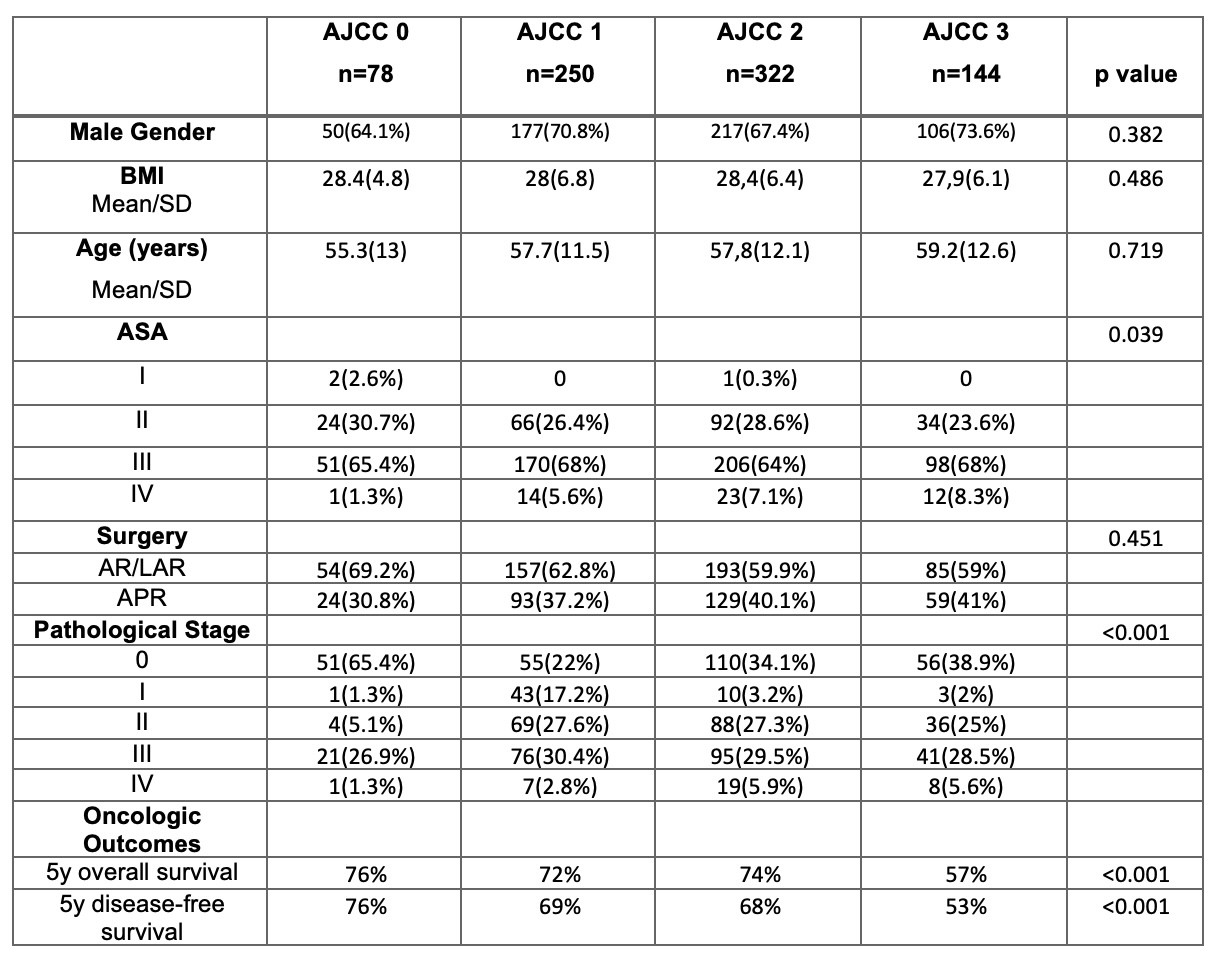
Results: A total of 794 patients met inclusion criteria: 78 (9.8%) AJCC 0, 250 (31.5%) AJCC 1, 322 (40.6%) AJCC 2, and 144 (18.1%) AJCC 3. In the cohort, patients were predominantly male (550, 69.3%), with a mean age at the time of the operation of 57,8 years (SD=12,1). The ASA classification was I in 3 patients (0.4%), II in 216 (27.2%), III in 525 (66.2%), and IV in 50 (6.2%). There were no differences among AJCC groups regarding gender (p=0.382), age (p=0.719), body mass index (p=0.486). Healthier patients exhibited better treatment response to neoadjuvant therapy (p=0.039). Surgical techniques were similar among the AJCC grades (p=0.451). As expected, more advanced pathological stages were found in partial and non-responders (p<0.001). Notably, higher AJCC regression grades were significantly associated with worse overall and disease-free survival (p<0.001). Multivariate Cox regression analysis confirmed AJCC tumor regression grade and pathological stage as independent factors for overall survival (p=0.005 and p<0.001, respectively) and disease-free survival (p=0.002 and p<0.001, respectively).
Conclusions: In this large single-center cohort, higher AJCC tumor regression grade following neoadjuvant therapy was associated with decreased overall and disease-free survival. These findings support incorporating AJCC tumor regression grade into postoperative risk stratification, follow-up planning, and individualized oncologic treatment decision-making for rectal cancer patients.
Back to 2026 Abstracts