METASTASECTOMY IMPROVES SURVIVAL IN MSI-HIGH CRLM PATIENTS IN THE IMMUNOTHERAPY ERA: A NATIONAL CANCER DATABASE ANALYSIS
Kevin Perez1, 2, Victor Dominguez1, 2, Maher Sraj2, David Caba Molina1, Vicente Ramos1, Aaron Saunders2, Emanuel Eguia21. Surgical Oncology, Riverside University Health System Medical Center, Moreno Valley, CA, United States.
2. Loma Linda University Health, Loma Linda, CA, United States.
Introduction
Microsatellite instability-High (MSI-H) metastatic colorectal cancer represents a biologically distinct subset characterized historically by poor response to cytotoxic chemotherapy and inferior survival after metastasectomy. The approval of immune checkpoint inhibitors (ICI) as first-line therapy for MSI-H metastatic colorectal cancer has changed the systemic management; however, the impact of ICIs - particularly in combination with hepatic resection for colorectal liver metastases (iCRLM) remains poorly defined. We aimed to evaluate whether overall survival (OS) among MSI-H iCRLM patients improved in the ICI era and to quantify the survival benefit associated with surgery and immunotherapy. We hypothesize that the OS in patients with iCRCLM and MSI-H tumors has significantly improved after the approval of ICIs.
Methods
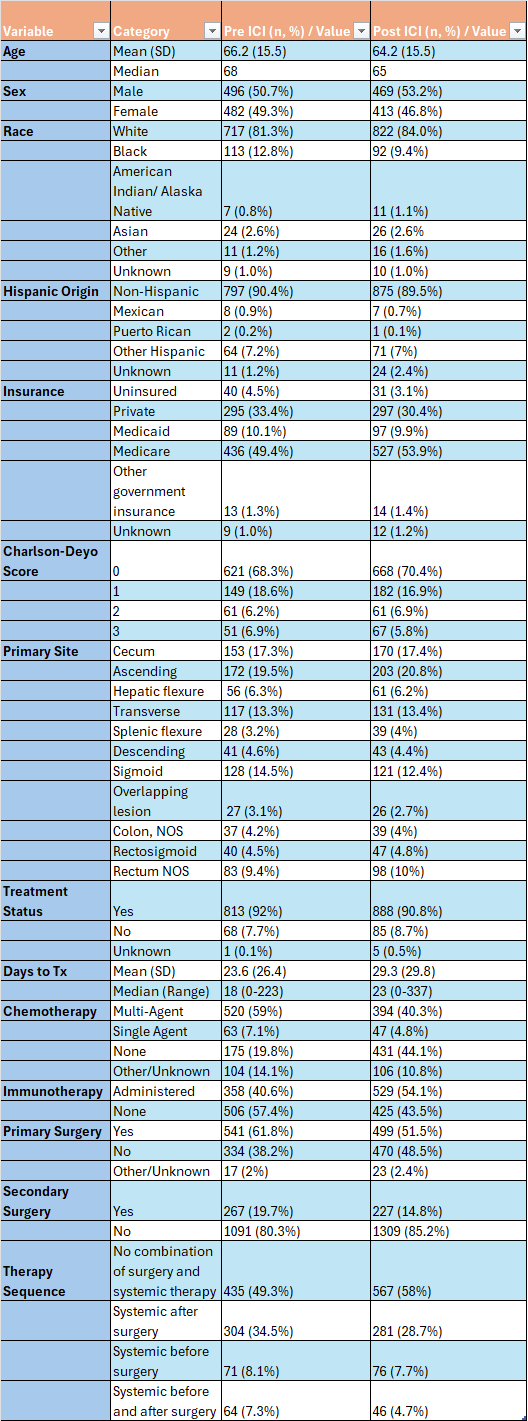
This was a retrospective cohort study using the National Cancer Database (2018-2023). Patients with MSI-H tumors and synchronous liver metastasis were included; those with extra-hepatic metastasis were excluded. The cohort (n= 1,860) was stratified into pre-ICI (2018-2020) and post-ICI (2021-2023) eras based on first line ICI approval. Propensity score matching was used to balance clinical and treatment variables. Survival was assessed using Kaplan-Meier analysis and Cox proportional hazard models, including stratification by treatment modality.
Results
MSI-H tumors constituted 5.4% of CRLM cases with documented MSI status. In the post-ICI era, chemotherapy use decreased (46.7% vs.67.6%), and first line ICI use increased (54.1% vs. 40.6%). Median OS improved significantly post-ICI (34.6 months, 95% CI 28.8 - 40.4) compared with pre-ICI (23.2 months, 95% CI 20.8 - 27.5). Among post-ICI patients, ICI therapy was associated with the highest survival benefit (HR 0.37, CI 0.31 - 0.45, p < 0.001)
Primary resection decreased in the post-ICI (51.5% vs. 61.8%) compared to the pre-ICI group. Rates of liver resection (14.8% vs 19.7%) followed a similar trend. In patients who received immunotherapy, the largest survival benefit was seen with liver resection in the post ICI era (HR 0.37, CI 0.23 - 0.59, p < 0.001). A modest effect was seen in cases without liver resection post-ICI compared to pre-ICI (HR 0.81 CI 0.67 - 0.97, p=0.022).
Conclusion
In this national analysis, survival for MSI-H iCRLM patients improved substantially after the adoption of first-line immunotherapy. Despite evidence of benefit, ICI utilization remains lower than expected. Importantly, the integration of hepatic resection with immunotherapy- regardless of treatment sequence results in the longest survival, supporting a multimodality approach in appropriate candidates. Efforts to improve access to both curative intent surgery and immunotherapy can meaningfully enhance outcomes for this unique molecular subset.

Back to 2026 Abstracts