
TRENDS AND OUTCOMES FOR SIMULTANEOUS CHOLECYSTECTOMY DURING BARIATRIC SURGERY OVER THE PAST DECADE
Paul T. Kröner*2, Michele B. Ryan1, Christopher C. Thompson1
1Brigham and Women's Hospital Department of Medicine, Boston, MA; 2Mayo Clinic's Campus in Florida, Jacksonville, FL
Introduction
Precipitous weight loss induced by bariatric surgical (BS) procedures (particularly Roux-en-Y gastric bypass [RYGB]) promotes the formation of gallstones. Cholelithiasis may in turn trigger later complications such as acute biliary pancreatitis, cholecystitis or cholangitis, which may be clinically challenging to address given the surgical anatomy. Therefore, much debate has sparked over the role of simultaneous cholecystectomy (CCY) and RYGB in terms of perioperative morbidity and mortality, and long-term cost-effectiveness. The aim of this study is to examine the trends of use for simultaneous RYGB and CCY over the past decade.
Methods
Retrospective observational study using the NIS 2008, 2011, 2014 and 2017, the largest public inpatient database in the US. All patients with ICD10CM procedural codes for RYGB were included. The primary outcome was the temporal trends in the use of simultaneous BS and CCY in the US. Secondary outcomes were the associated trends in post-operative mortality, morbidity and resource utilization in this patient population. Multivariate regression analyses were used to adjust for gender, age, Charlson Comorbidity Index, income in patient zip code, hospital region, location, size and teaching status.
Results
The total number of patients undergoing RYGB in the four studied years was 258,462. The mean age of patients was 47.3 years. The proportion of female patients was 75.60%. For the primary outcome, out of the 92,488 in 2008, 6,334 (6.85%) underwent simultaneous CCY, while in 2017 out of the 45,831 patients undergoing RYGB, 2,607 (5.69%) underwent simultaneous CCY (Table 1). On multivariate analysis, patients undergoing RYGB in 2017 displayed adjusted odds of 0.63 (95%CI: 0.42-0.83, p<0.01) of undergoing simultaneous CCY compared to 2008. For the secondary outcomes, inpatient mortality in patients undergoing simultaneous BS and CCY has not changed from 2008 to 2017. However, the odds of morbidity during the admission for the procedures has increased throughout the study period. There was no significantly different inflation-adjusted total charges or LOS for patients in 2017 compared to 2008. All outcomes are displayed in Table 2.
Conclusion
Performing simultaneous CCY during RYGB has decreased both numerically and proportionately in the past decade. Patients undergoing simultaneous CCY during RYGB showed increased odds of morbidity in 2017 compared to 2008, while mortality and resource utilization has remained unchanged. These findings may reflect the fact that patients undergoing simultaneous CCY during RYGB may have increased baseline comorbidity burden, and may also support current evidence suggesting a higher morbidity in patients undergoing these procedures simultaneously.
Table 1: Crude number of BS and CCY by year.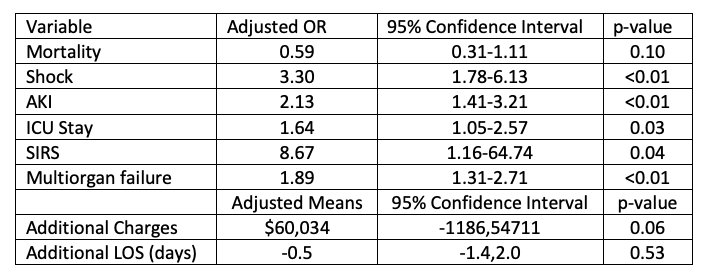
Table 2: Adjusted odds and means of undergoing simultaneous BS and CCY in 2017 compared to 2008.
Back to 2021 Abstracts