
IMPLEMENTATION OF AN ENHANCED RECOVERY PATHWAY RESULTS IN DECREASED LENGTH OF STAY AFTER GASTRECTOMY
Anitha Kammili*, Jonathan Cools-Lartigue, Lorenzo E. Ferri, Carmen L. Mueller
McGill University Health Centre, Montreal, QC, Canada
Background
Enhanced recovery after surgery (ERAS) protocols aim to decrease surgical stress and optimize post-operative recovery. However, concern remains that such protocols may lead to increased complications. Therefore, the aim of this study was to evaluate surgical outcomes before and after implementing an ERAS protocol for patients undergoing anatomical gastrectomy.
Methods
Patients undergoing anatomical, non-bariatric gastrectomy with anastomoses between 2010-2019 at McGill University Health Centre were identified and data extracted from a prospectively collected database. Patient outcomes and adherence to gastrectomy-specific ERAS protocol were compared before (pre-ERAS: 2010-2015) and after (post-ERAS: 2016-2019) implementation. Mann Whitney U, Fisher Exact, and χ2 tests were utilized to compare groups. Data are presented as median [interquartile range].
Results
A total of 212 patients were included (pre-ERAS: 100 (47%), post-ERAS: 112 (53%)). Patient age, sex, comorbidities, tumor location, and histology were comparable between groups. Nutrition counselling, avoiding Dobhoff tube and abdominal drains, and introducing feeds by post-operative day 1 were the most frequently adhered to components of the protocol (Table 1). Median length of stay decreased by two days (pre-ERAS: 6 [4-10] days, post-ERAS: 4 [3-7] days; p<0.001) after ERAS implementation. The incidence of major complications (Clavien-Dindo 3-4) within 30 days of surgery (pre-ERAS: 22 (22%), post-ERAS: 25 (26%); p=0.68), emergency room visits (pre-ERAS: 15 (15%), post-ERAS: 23 (21%); p=0.10), readmissions (pre-ERAS: 8 (8%), post-ERAS: 16 (14%); p=0.19), and mortality (pre-ERAS: 4 (4%), post-ERAS: 2 (2%); p=0.68) did not vary over the study period.
Conclusion
Implementing an ERAS gastrectomy protocol decreased the median length of stay after anatomical gastrectomy without impacting morbidity, mortality, and readmissions.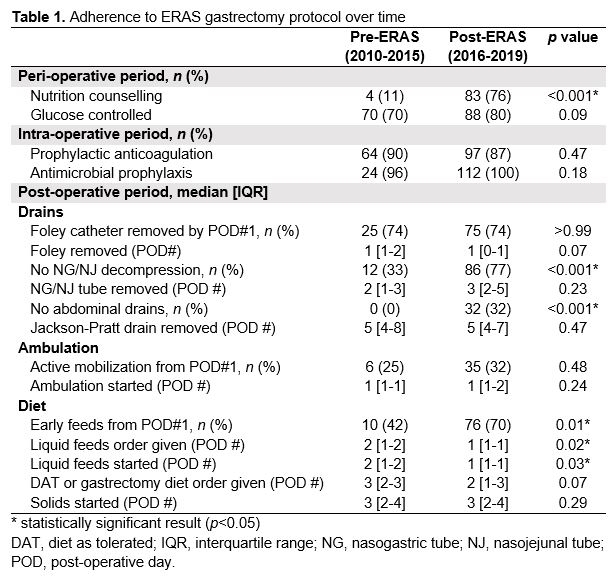
Back to 2021 Abstracts