
PLATELET-TO-LYMPHOCYTE RATIO AS A MARKER OF DISEASE PROGNOSIS IN ESOPHAGEAL ADENOCARCINOMA
Alexander J. Calderone*, Yaseen Al Lawati, Jose L. Ramirez-Garcialuna, Aroub Alkaaki, Carmen L. Mueller, Jonathan Spicer, Lorenzo E. Ferri, Jonathan Cools-Lartigue
McGill University Faculty of Medicine, Montreal, QC, Canada
Background: Markers of cancer associated systemic inflammation have been implicated as prognostic indicators in several malignancies. The neutrophil-to-lymphocyte ratio (NLR) is one such indicator whose dynamic changes during treatment were found to be associated with patient survival in patients with esophageal adenocarcinoma. The platelet-to-lymphocyte ratio (PLR) is another element whose significance has yet to be fully characterized in this patient group. The aim of this study was to correlate dynamic alterations in PLR values with overall and disease free survival in patients with resectable gastro-esophageal cancer.
Methods: Following ethics approval, a retrospective single center cohort review was conducted. A prospectively entered database of patients operated between 2005 to 2018 for gastro-esophageal adenocarcinoma was queried. Peripheral blood samples were collected prior to treatment for establishment of a baseline PLR value followed by a second sample collected 1-4 months after surgery.
Patients were stratified based on low or high PLR. These were then separated into one of four groups based on the change in their PLR values between baseline and post-op (low-low, low-high, high-low and high-high). Optimal PLR cut-off values for high and low categories were obtained from receiver operating characteristic (ROC) curves. Kaplan-Meier plots and log-rank tests were used to compare survival. Wilcoxon Rank Sum test was used to compare the median values of PLR between groups. A p-value of 0.05 was considered significant. Statistical analyses were performed using R (v.4.0.1, R Foundation for Statistical Computing, 2020). The primary outcomes of the study were overall survival and disease free survival. These were compared between low and high PLR groups and subsequently, between the four PLR trend groups.
Results: A total of 330 patients were included. Mean age was 65.6 years with a male preponderance (82%). 74.8% of patients presented with locally advanced disease (cT3N+) and 65.2% received neoadjuvant chemotherapy. There was a significant difference in overall survival between low and high PLR groups both at baseline (p = 0.0032) and post-op (p < 0.0001) (figure 1). A significant difference in disease free survival between both groups at baseline (p = 0.026) and post-op (p < 0.0001) was also reported. Patients whose PLR remained stratified as low at both baseline and after surgery had the best overall survival and disease free survival out of the four groups being compared (figure 2).
Conclusion: Patients who demonstrated an elevated PLR at baseline or following surgery exhibited poor overall survival and disease free survival outcomes compared to those with low PLR. These values may thus be used as a prognostic marker for patients with resectable gastro-esophageal adenocarcinoma.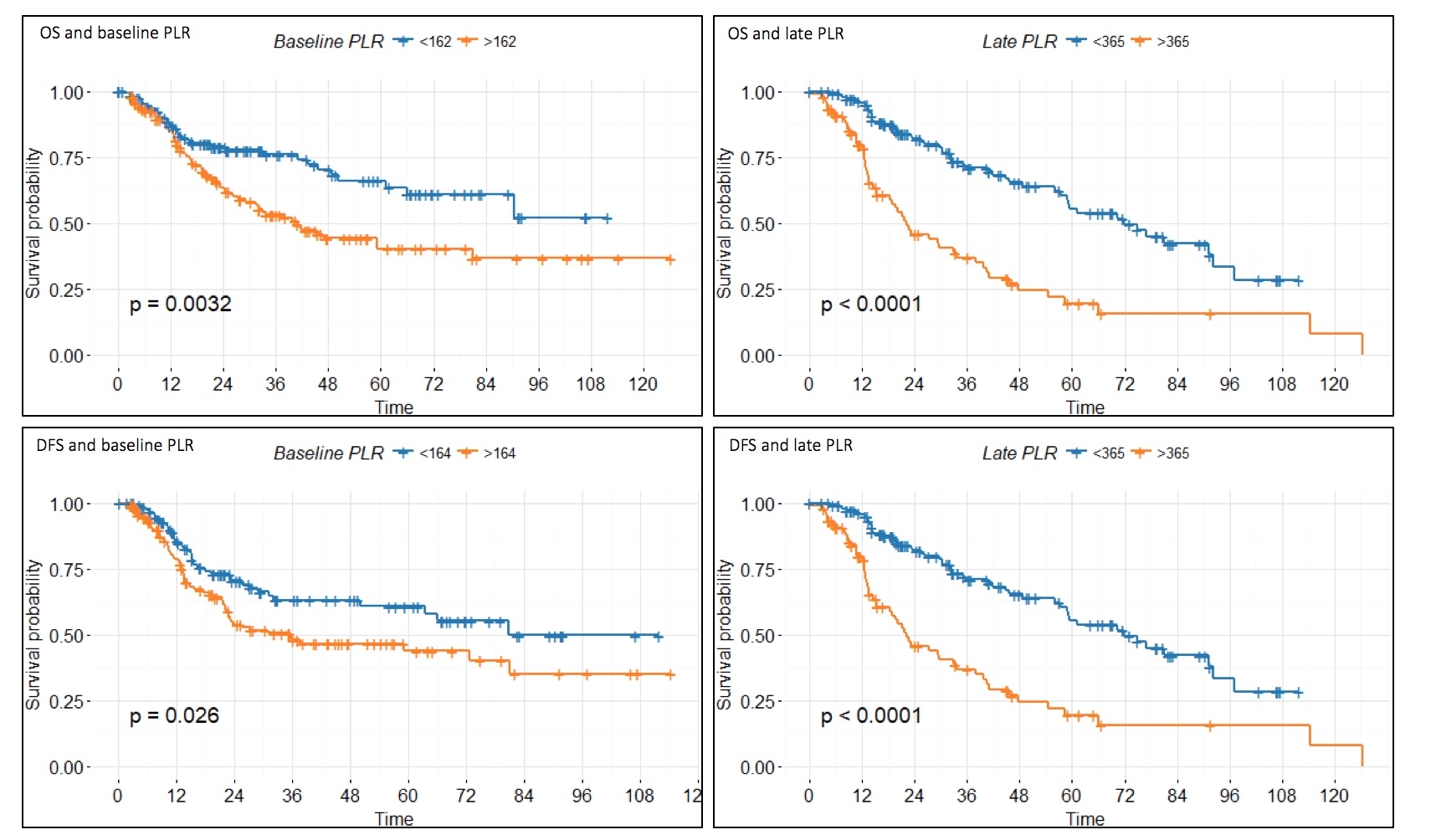
Survival and disease free survival comparison between low and high PLR stratified patients at baseline and post-op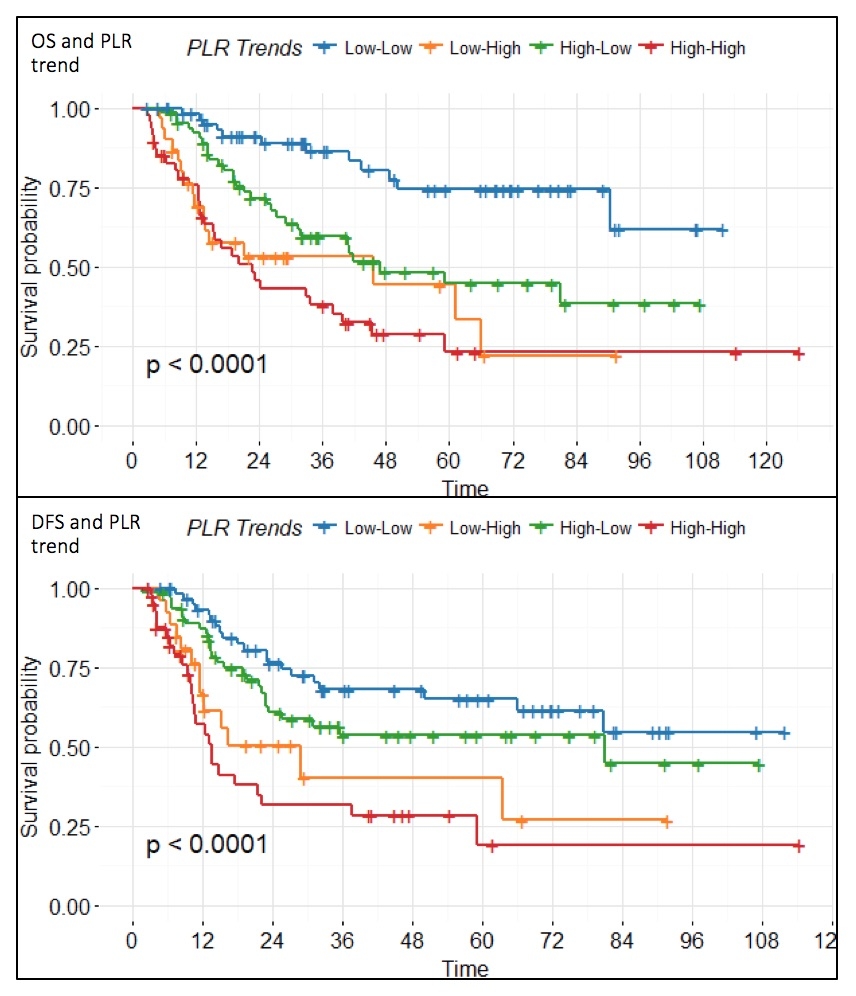
Survival and disease free survival comparison between four PLR trend stratified groups
Back to 2021 Abstracts