
DISCHARGE TIMING AFTER OSTOMY CONSTRUCTION: IS SHORT LENGTH OF STAY ASSOCIATED WITH INCREASED READMISSIONS?
Mary G. Smithson*, Tara Wood, Karin M. Hardiman, Drew J. Gunnells, Daniel I. Chu, Robert H. Hollis
The University of Alabama at Birmingham, Birmingham, AL
Background: Adoption of enhanced recovery pathways has led to decreasing length of stay following colorectal surgery; however, this may put new pressures on patients with a new ostomy who often receive inpatient ostomy education. Whether shorter length of stay is associated with higher readmissions for these patients is unknown. We hypothesized that patients undergoing ostomy construction with an uncomplicated hospital course who are discharged within 2 days of surgery have a higher risk of readmission than patients discharged 3-5 days after surgery.
Methods: The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried for patients undergoing ostomy construction from 2016-2018. Patients with postoperative length of stay longer than 5 days, non-elective operation, outpatient surgery, or who experienced any inpatient complication were excluded. Patients were divided into early discharge (1-2 days) and late discharge (3-5 days). The primary outcome was readmission within 30 days of surgery. Univariate analysis was performed using chi-square and Kruskal-Wallis tests. A multivariable logistic regression model of 30-day readmission including patient and procedure related factors was used to assess the relationship between early discharge and readmission. As a sensitivity analysis, we performed 1:1 propensity score matching between patients in the early and late discharge groups and compared 30-day readmission rates.
Results: We identified 13,202 patients undergoing ostomy construction including 2,555 (19.3%) in the early discharge group and 10,647 (80.6%) in the late discharge group. The groups were similar in age and gender. Patients in the late discharge group were more likely to have undergone LAR/APR/Hartman's (62.2% vs 34.2%), total colectomy (17.7% vs 16.0%), and partial colectomy (3.3% vs 2.7%), whereas patients with early discharge more often underwent simple colostomy (10.9% vs 30.7%) or ileostomy construction (5.8% vs. 16.4%). On unadjusted analysis, readmissions were lower in the early discharge group (early:11.1% vs. late:14.2%; p=<0.01; Figure). Median days from discharge to readmission were similar between the two groups (early: 6 days vs. late: 7 days; p=0.26). On multivariable analysis, the early discharge group was associated with lower odds of 30-day readmission compared to the late discharge group (OR 0.84, 95%CI 0.73-0.97). In the propensity score matched cohort, there was no significant difference in readmission rates between early and late discharge groups (early:11.3% vs late:13%, p=0.07).
Conclusion:
Select patients with a new ostomy can be discharged home within 2 days of surgery without a significant increase in readmission. Future studies are needed to better understand the processes that facilitate early discharge for patients with a new ostomy.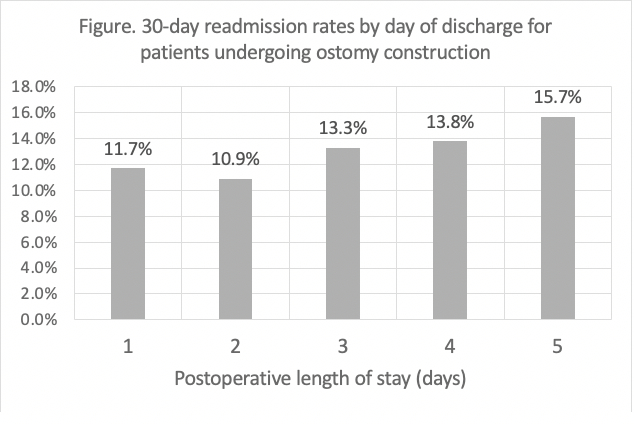
Back to 2021 Abstracts