
THE ROLE OF EXTENDED PORTAL LYMPHADENECTOMY DURING HEPATECTOMY FOR INTRAHEPATIC CHOLANGIOCARCINOMA
Thomas K. Maatman*, John Aversa, Katelyn Flick, Shelby L. Allen, Eugene P. Ceppa, Attila Nakeeb, Trang K. Nguyen, C. Max Schmidt, Nicholas J. Zyromski, Michael G. House
Indiana University School of Medicine, Indianapolis, IN
Introduction:
Intrahepatic cholangiocarcinoma (IHC) is the second most common primary hepatic malignancy, but a knowledge gap exists as to which factors influence accurate staging after hepatic resection for IHC. Recovery of at least six lymph nodes (LN) during operation for IHC remains as the current recommendation by the American Join Committee on Cancer (AJCC). The purpose of this study was to examine whether extended portal lymphadenectomy is associated with improved staging accuracy for patients with resectable IHC.
Methods:
All patients undergoing hepatectomy for resectable IHC at a single institution between 2006 and 2018 were included. Sociodemographic, comorbidities, and perioperative outcomes were recorded prospectively in an institutional database. Portal lymphadenectomy was performed routinely by one surgeon and selectively in the remaining cases. Surgical pathology was staged retrospectively according to the AJCC 8th edition staging system. Major morbidity was defined as Clavien-Dindo grade III or higher complications. Patients dying within 30-days postoperatively were excluded from disease-free survival (DFS) and overall survival (OS) analysis. Patients were divided into two groups according to the number of LN recovered: less than six (<6) and six or more (6+).
Results:
A total of 95 patients underwent hepatectomy (+/- portal lymphadenectomy) for resectable IHC. The mean age was 65'±11 years and 48 (51%) patients were male. 87 (92%) patients underwent resection without neoadjuvant therapy; the remaining 8 patients received preoperative therapy including chemotherapy alone in six (6%) patients, radiotherapy alone in one (1%), and chemotherapy with hepatic artery radioembolization in one (1%). Left hepatectomy or left trisectionectomy was performed in 39 (41%) patients and right hepatectomy or right trisectionectomy in 37 (39%). Partial hepatectomy was performed in the remaining 19 (20%) patients. The mean tumor size was 5.6'±3.9 cm. A median of 5 (range, 0-23) LN were recovered. Six or more LN were recovered in 45 (47%) patients. Overall morbidity and major morbidity were 42% and 31%, respectively. No differences were observed in overall morbidity (<6 = 38% vs. 6+ = 47%, p = 0.4) or major morbidity (26% vs. 36%, p = 0.3) between groups. 30-day perioperative mortality was observed in 7 (7%) patients and was similar between groups (12% vs 2%, p = 0.07). Median DFS and OS were 8.8 months and 14.7 months, respectively. A comparison of DFS and OS according to extent of portal lymphadenectomy among each AJCC stage is shown in Table 1.
Conclusions:
During hepatectomy for intrahepatic cholangiocarcinoma, extended lymphadenectomy with recovery of six or more portal lymph nodes is recommended for patients with early stage IHC.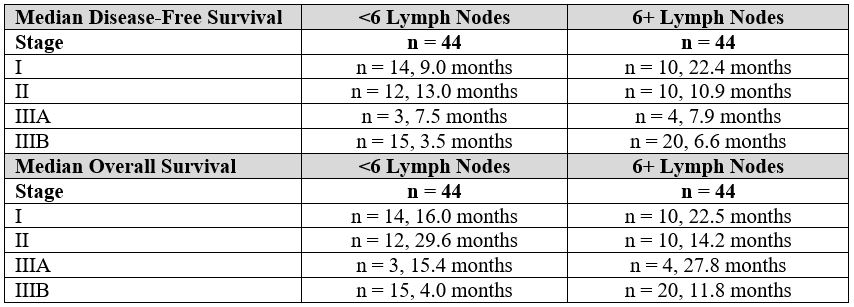
Table 1. Median disease-free and overall survival between patients with less than 6 lymph nodes (<6 LN) and six or more lymph nodes (6+ LN) evaluated. Note: statistical comparison was not performed given the number of patients included in the analysis.
Back to 2021 Abstracts