
EVERY DROP MATTERS: INTRAOPERATIVE FLUIDS DURING HEPATECTOMY AND POSTOPERATIVE ILEUS
Cameron Gaskill*, Bradford J. Kim, Timothy E. Newhook, Elsa M. Arvide, Whitney L. Dewhurst, Teresa L. Phan, Jenilette . Cristo, Hop Tran Cao, Thomas Aloia, Yun Chun, Jean-Nicolas Vauthey, Ching-Wei D. Tzeng
The University of Texas MD Anderson Cancer Center Division of Surgery, Houston, TX
Introduction: Postoperative ileus is a major contributor to post-hepatectomy length of stay (LOS). We sought to analyze the association between intraoperative fluid resuscitation and postoperative ileus to identify potential guidelines for standardization.
Methods: We studied consecutive patients undergoing isolated hepatectomy (1/2017-6/2019), using a single-institution prospective database. Patient information, perioperative details, and 90-day ACCORDION complications were verified by a faculty surgeon. Intraoperative fluid resuscitation was the sum of all crystalloid, colloid, and blood products. Ileus was defined as nasogastric decompression or radiographic confirmation.
Results: 496 patients (median age 57 years) were analyzed. 7.5% (n=37) experienced postoperative ileus. Comparing patients with ileus versus those without, there were no differences in body mass index (BMI, p=0.160), mean operative length (p=0.058), mean Pringle time (p=0.769), and Kawaguchi-Gayet classification (p=0.983). Ileus was associated with major complications (p=0.033), biloma/organ space infections (p=0.004), and resultant increased LOS (10.1 vs. 4.5 days;p<0.001). Acute kidney injury (Creatinine >1.5) was rare (9/496 patients;p=0.674). Mean intraoperative resuscitation was 2.2L for patients who went on to develop ileus versus 1.6L for those who did not (p=0.002). In patients who received <1.5L, ileus occurred in only 1.7% (Figure). After controlling for operative length, major complication, and BMI, each additional liter received intraoperatively was associated with 79% increased odds of developing ileus (OR-1.79;95% CI-1.16-2.76,p=0.009).
Conclusion: Excessive intraoperative intravenous fluid is associated with postoperative ileus and resultant length of stay. To mitigate ileus risk, a simple rule to consider is to limit all hepatectomies to <1.5L of intraoperative fluid.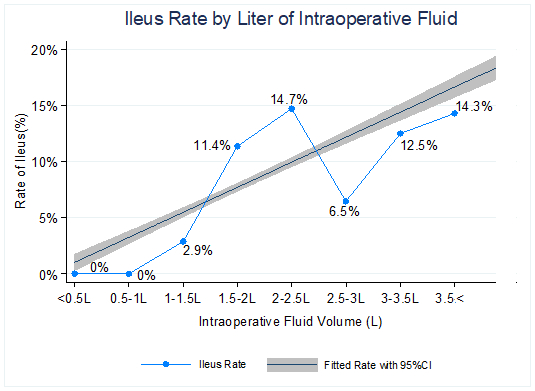
Back to 2021 Abstracts