
SURVIVAL IN PATIENTS WITH COLORECTAL LIVER METASTASES IS ASSOCIATED WITH MULTIMODALITY CAPACITY OF THE TREATING FACILITY
Anai N. Kothari*, Caitlin A. Hester, Ching-Wei D. Tzeng, Timothy E. Newhook, Yun Chun, Aloia Thomas, Jean-Nicolas Vauthey, Hop Tran Cao
Surgical Oncology, MD Anderson Center, Houston, TX
Introduction:
A multidisciplinary approach optimizes outcomes for patients with colorectal liver metastases (CLM) as treatment can involve surgery, ablation, radiation, chemotherapy, and more recently, transplant. However, the availability of these resources is not uniform across treating facilities. Therefore, we sought to measure variation in availability of liver-directed therapies and association with survival for patients with CLM.
Methods:
The National Cancer Database was used to identify patients with stage IV colon and rectal cancers between 2010 and 2015. Only patients with hepatic metastases were included. Facilities were stratified by the cumulative number of therapeutic modalities offered to patients with liver cancer using the NCDB liver participant use file: surgery, ablation, radiation, chemotherapy, transplant. Median overall survival was calculated using Kaplan-Meier method and adjusted analyses were performed using shared frailty survival models.
Results:
47,121 patients met our inclusion criteria and were treated at 1,296 facilities. 440 patients received treatment at facilities with 1 modality, 2,364 with 2 modalities, 8,250 with 3 modalities, 19,641 with 4 modalities, and 16,426 with 5 modalities. A total of 222 facilities offered all 5 modalities of treatment. Median survival ranged from 16.4 months (1 modality) to 23.9 months (5 modalities) (Figure). After adjustment for patient factors, disease site, and facility characteristics, treatment at facilities with 4 (HR 0.87 [0.76 - 0.99]) or 5 (HR 0.76 [0.66 - 0.88]) available modalities was associated with improved survival.
Conclusion:
Treatment at facilities that offer more liver-directed therapeutic options is associated with improved survival in patients with CLM, suggesting that the care delivery environment significantly impacts outcomes. However, less than 40% of patients are treated at the highest resourced facilities. These data support the benefit of a multidisciplinary approach to the management of patients with CLM and offer a target for improving survival in this population.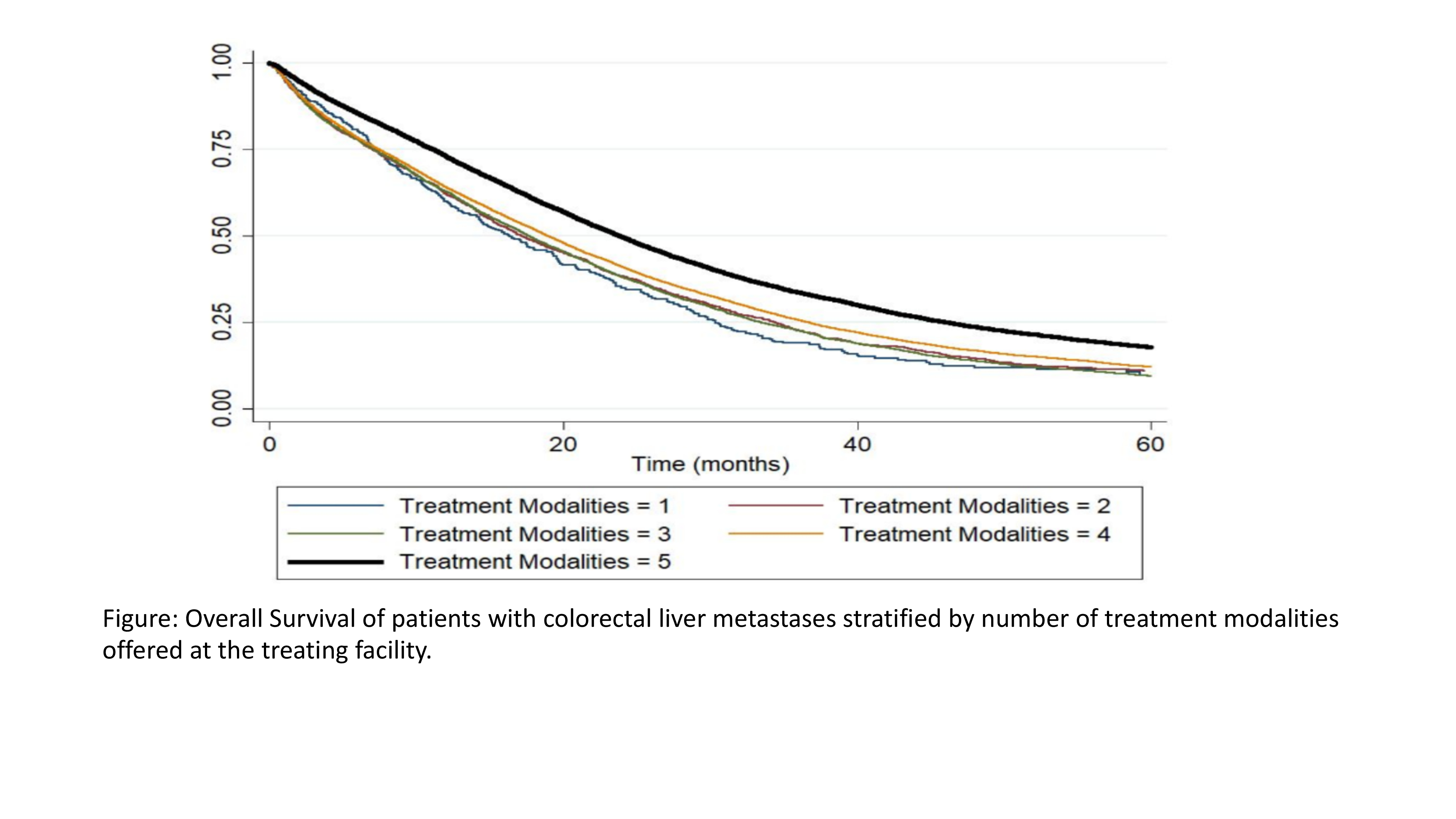
Back to 2021 Abstracts