
DYNAMIC RISK PREDICTION OF MORBIDITY AND MORTALITY POST BARIATRIC ROUX-EN-Y-GASTRIC BYPASS SURGERY
Suha Jabak*1, Fadel Alturki1, Nancy Mikati2, Mostafa M. Abohelwa3, Yasser H. Shaib1
1American University of Beirut, Beirut, Lebanon; 2University of Pittsburgh Medical Center, Pittsburgh, PA; 3Texas Tech University System, Lubbock, TX
Objectives: The aim of this study was to identify the risk factors predicting morbidity and mortality post laparoscopic bariatric Roux-en-Y gastric bypass surgery.
Methods: Data was collected retrospectively from the NSQIP database (2005-2013). Patients who had laparoscopic Roux-en-Y gastric bypass surgery were included. Exclusion criteria included patients with BMI < 30, age > 90, as well as patients who had disseminated cancer or had undergone emergent surgeries. Our primary endpoints were major morbidity and mortality post laparoscopic roux-en-y surgery. Major morbidity was defined as having any of the following: re-admission, cardiac arrest, myocardial infarction, stroke, pulmonary embolism and deep tissue infection. A dynamic multivariate regression model was used to study the significant predictors of the primary outcomes. It included pre-operative, intra-operative, and postoperative risk factors. A Receiver Operating Characteristic (ROC) curve was used to study the discriminatory power of the model. A risk calculator and risk ruler were generated to predict the morbidity and mortality based on the results.
Results: A total of 66,297 patients were included. More than 50% had a BMI more than 45, and the majority of the patients were males (79.6%) in the age group of 45-60 (61.7%). Older age, BMI > 40, smoking, chronic steroid use, along with obesity-related morbidities such as impaired functional status, diabetes mellitus, congestive heart failure, kidney disease, and hypertension were found to be significant predictors of morbidity and mortality. Pre-operative characteristics of high American Society of Anesthesiologists classification, anemia, concurrent hiatal hernia surgery or cholecystectomy were also found to be strong predictors of surgical mortality and morbidity. ROC discriminatory power of pre-operative risk factors for mortality and morbidity were 0.801 and 0.586, respectively. After adding operative risk factors of prolonged surgery time of more than 2.75 hours and increased number of transfusions needed, the ROC discriminatory power for mortality and morbidity were 0.822 and 0.611 respectively. The ROC discriminatory power became 0.879 for mortality and 0.709 for morbidity after adding postoperative risk factors such as urinary tract infections (UTIs), pneumonia, reintubation, prolonged duration of intubation, deep vein thrombosis (DVT), and prolonged length of stay of more than five days.
Conclusion:
The new dynamic risk calculator has significant discriminatory power for predicting mortality and morbidity post laparoscopic Roux-en-Y gastric bypass surgery. Identifying high risk patients will help optimize their pre-operative conditions as well as their post-operative surgical care.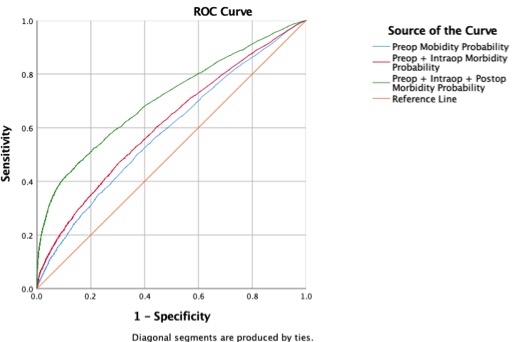
The receiver operating charactersitic curves(ROCs) of risk scores for morbidity post bariatric roux en y gastric bypass surgery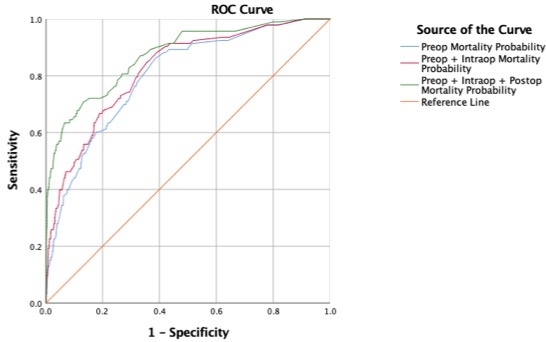
The receiver operating characteristic curves (ROCs) of risk scores for mortality post bariatric roux en y gatsric bypass surgery
Back to 2021 Abstracts