
COMPARISON OF ADAPTED ENHANCED RECOVERY AFTER SURGERY PATHWAY VERSUS STANDARD CARE IN PATIENTS UNDERGOING EMERGENCY LAPAROTOMY FOR PERFORATION PERITONITIS - A RANDOMIZED CONTROLLED TRIAL
Pranavi A. Ravichandar*1, Vikram Kate1, Sathasivam Sureshkumar1, Thulasingam Mahalakshmy2, Pankaj Kundra3
1Department of Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry, India; 2Department of Preventive and Social Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry, India; 3Department of Anesthesia and Critical Care, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry, India
Introduction: Enhanced Recovery after Surgery (ERAS) pathways have an uncertain role in emergency settings, with the question of safety in applying them to a population that is sicker than elective patients, often presenting with intra-abdominal infection; and the feasibility of implementing pre-operative and some intra-operative elements. Some studies have studied ERAS protocols in a modified form to circumvent this. To the best of our knowledge, there have been no randomized controlled trials studying ERAS in perforation peritonitis across the GI tract, despite it being a common surgical emergency. This study was carried out to investigate the feasibility and efficacy of adapted ERAS pathways in patients undergoing emergency surgery for perforation peritonitis across the GI tract.
Methods: This was a single-center, prospective, open-labeled, superiority, randomized controlled trial carried out in a tertiary care hospital. All consecutive patients over 18 years of age with perforation peritonitis planned for emergency laparotomy based on clinical and adjunctive investigations were included. Patients with refractory shock, ASA class 4E, polytrauma patients with associated other intra-abdominal organ injuries, patients with localised peritonitis, and pregnant patients were excluded. Eligible patients were randomly assigned in 1:1 ratio to either the standard care or adapted ERAS groups using a serially numbered opaque sealed envelope. Block randomization was done once decision to operate was taken, with block sizes of 4 and 6 (Table 1). Primary outcome was the length of hospitalization (LOH). Secondary outcomes were functional recovery parameters, morbidity, comparing the sites of perforations in the upper and lower GI tracts, and to identify factors responsible for delayed discharge within the adapted ERAS group. The study was registered at www.ctri.gov.in (CTRI/2019/02/017537).
Results: A total of 120 patients were included in the study period between October 2018 and June 2020, and were randomized into standard care group - 59 patients, and adapted ERAS group- 61 patients (Table 2). The two groups were comparable in terms of demographic and clinicopathological characteristics. LOH in adapted ERAS group was significantly shorter (3 days, p<0.001) when compared to the standard care group. Patients in the adapted ERAS group had significantly earlier recovery (days) with a reduction in the time to first flatus (1.38, p<0.001), first stool (1.7, p<0.001), first fluid diet (3.08, p<0.001) and solid diet (3.7, p<0.001). Urinary catheter (3.72, p<0.001) was also removed significantly early in adapted ERAS group. (Table 2)
Conclusion: Adapted ERAS pathways are safe and feasible in patients undergoing emergency surgery for perforation peritonitis, with a considerable reduction in LOH, and without an increase in the rate of complications.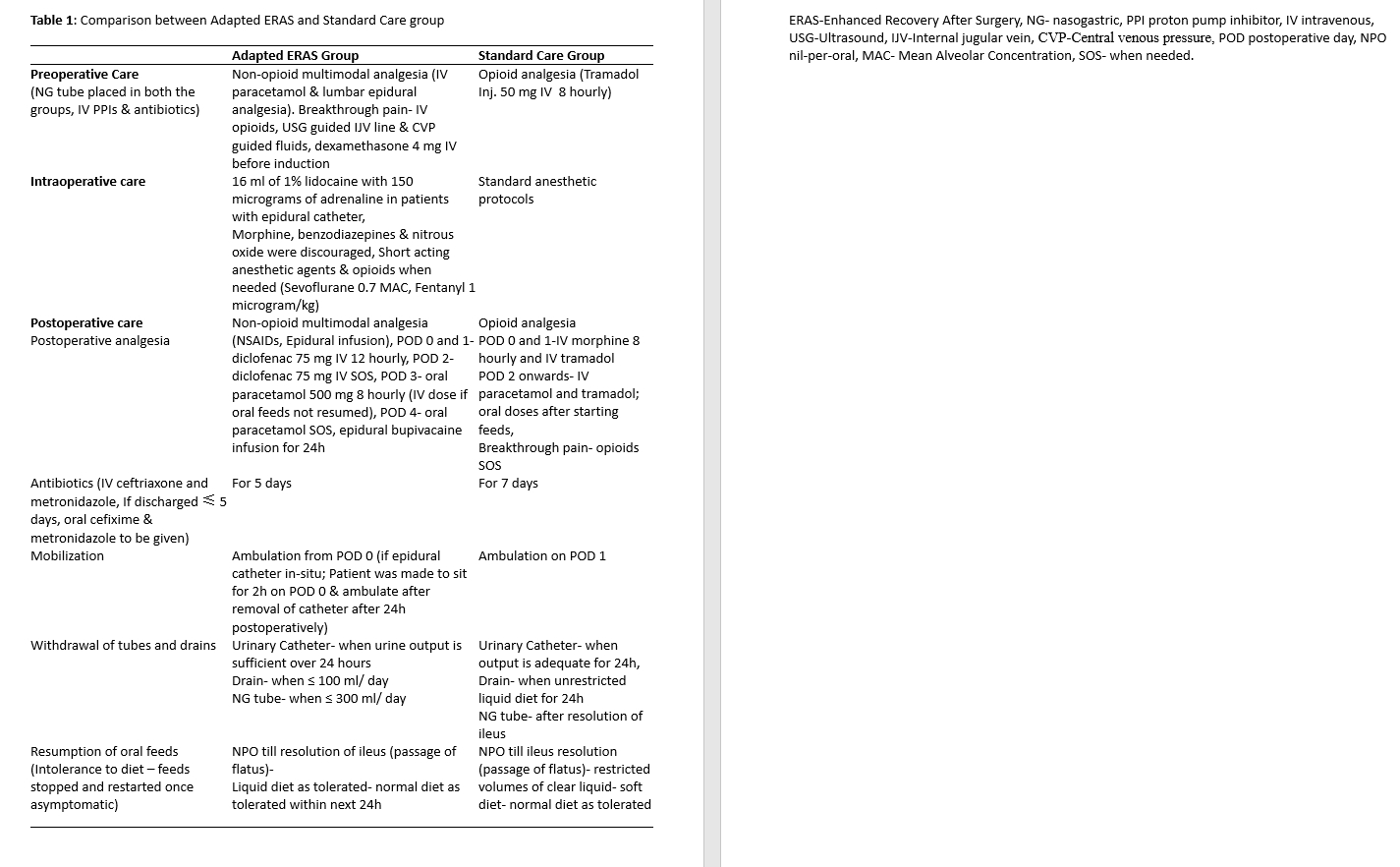
Table 1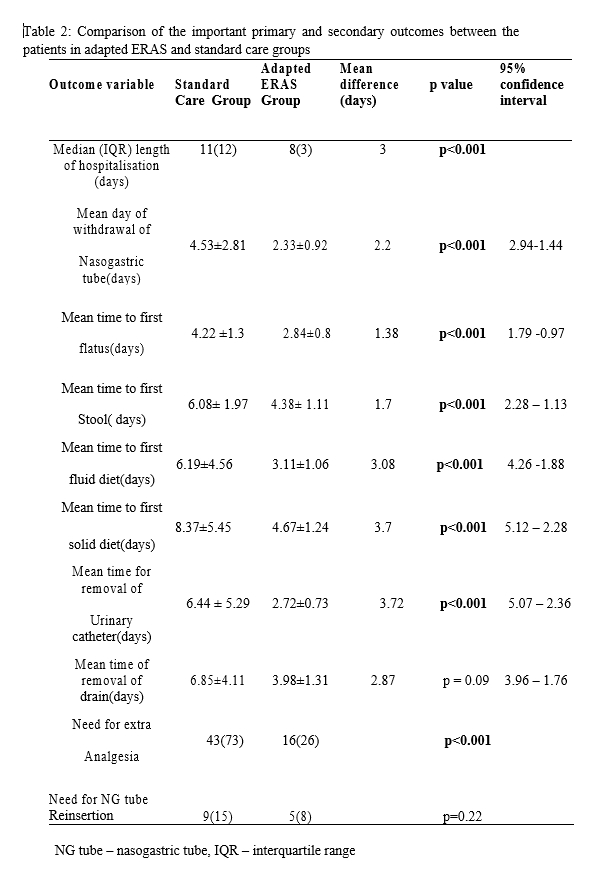
Table 2
Back to 2021 Abstracts