
PANCREATIC TAIL VOLUMETRICS: A NOVEL APPROACH FOR SURGICAL DECISION-MAKING IN DISCONNECTED PANCREATIC DUCT SYNDROME
Shelby L. Allen*, Mackenzie K. Madison, Sean P. McGuire, Eugene P. Ceppa, Michael G. House, Attila Nakeeb, Trang K. Nguyen, C. Max Schmidt, Temel Tirkes, Nicholas J. Zyromski
Department of Surgery, Indiana University School of Medicine, Indianapolis, IN
Introduction: Disconnected pancreatic duct syndrome (DPDS) is a challenging sequela of necrotizing pancreatitis (NP). The pancreatic remnant tail size is variable, and splenic vein thrombosis with left-sided portal hypertension is common. Many DPDS patients require operative management, either drainage or resection; however, no objective metrics exist currently with which to predict optimal definitive operative treatment. We therefore investigated radiographic volumetric measurement of the pancreas tail remnant and hypothesized that larger remnant tail volumes would be associated with an increased need for operative intervention.
Methods: Query of a prospectively-maintained NP database identified those with DPDS. Cross-sectional imaging obtained on or near the time of diagnosis of DPDS was analyzed using Intellispace (Phillips corporation, Andover, MA, USA) to measure the volume of the pancreatic tail remnant to the left of the ductal disconnection. Pancreas tail volume was evaluated with relation to surgical management pathways.
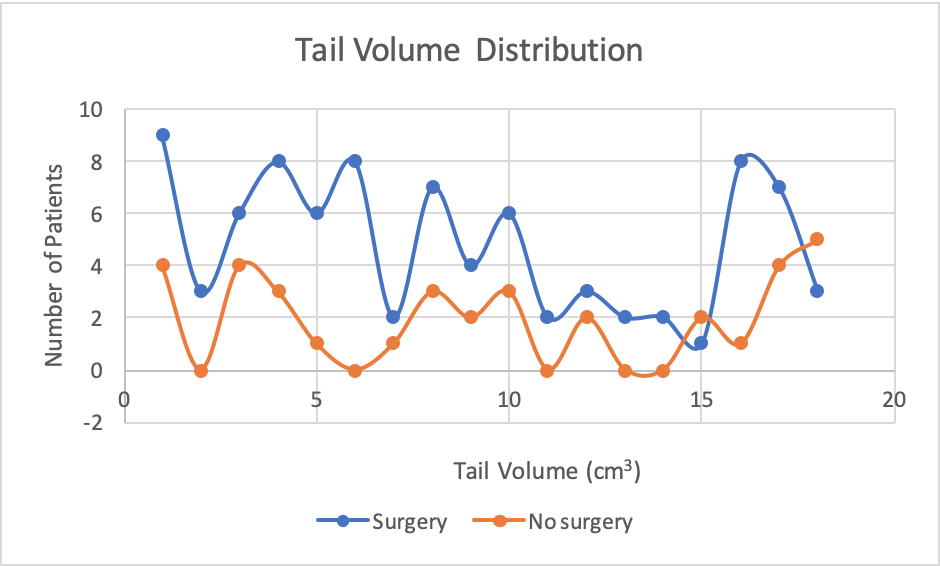
Results: Among 330 DPDS patients, 123 had appropriate imaging for analysis. Of those patients, 35 were managed nonoperatively, and 88 had surgical treatment for DPDS. The mean tail volume for patients managed medically was 12.7'±2.3 cm3 compared to 9.1'±0.9 cm3 for those undergoing surgical intervention (p=0.075). Operative intervention included 45 distal pancreatectomies and 43 drainage procedures (cystgastrostomy, cystjejunostomy, lateral pancreaticojejunostomy, external drainage). The mean tail volume in patients undergoing resection was 7.89'±1.0 cm3, vs 10.1'±1.5 cm3 in patients undergoing drainage procedures (p=0.105). Patients undergoing resection had a significantly longer time to intervention than patients undergoing drainage (133 days vs 49 days, p=0.03). Patients with pancreas tail remnant volume greater than 20 cm3 were significantly less likely to undergo an operative procedure than patients with tail volumes less than 20 cm3 (53% vs 75%, p=0.05).
Conclusion: Pancreatic tail remnant > 20 cm3 is associated with successful non-operative management in DPDS. Pancreas tail remnant volumetrics are a novel, useful tool for selecting DPDS treatment.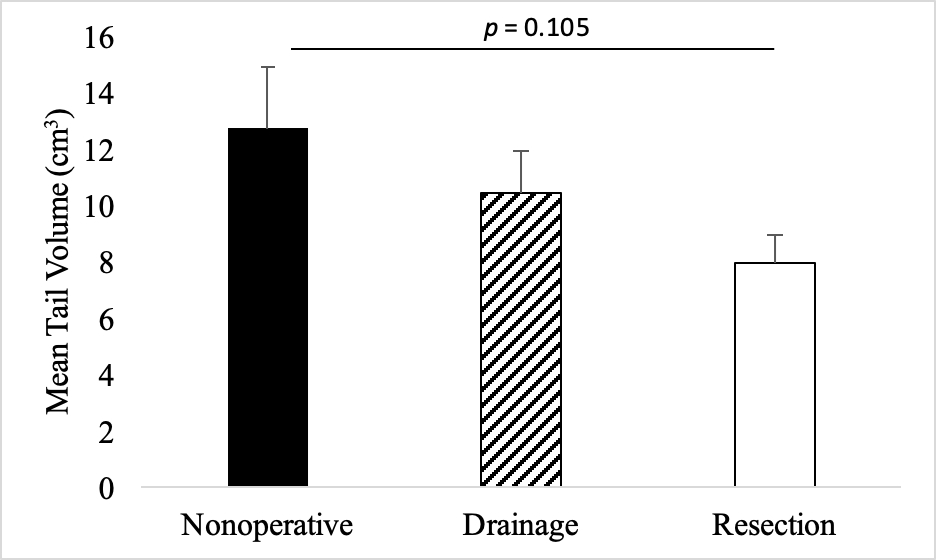
Back to 2021 Abstracts