
RACE, AGE, GENDER, AND INSURANCE STATUS: A COMPARATIVE ANALYSIS OF ACCESS TO AND QUALITY OF GASTROINTESTINAL CANCER CARE
Omid Salehi*1, Eduardo A. Vega1, Christopher Lathan1, Daria M. James1, Olga Kozyreva1, Sylvia V. Alarcon1, Onur C. Kutlu2, Beth Herrick3, Claudius Conrad1
1Saint Elizabeth's Medical Center, Brighton, MA; 2University of Miami School of Medicine, Miami, FL; 3University of Massachusetts Medical School, Worcester, MA
BACKGROUND: Socioeconomics, demographics, and insurance status play roles in healthcare access. Considering the limited resources available, understanding the relative impact of disparities helps prioritize programs designed to overcome them. This study evaluates GI cancer care disparity by comparing the impact of different patient factors across oncologic care metrices.
METHODS: A multi-institutional prospectively maintained cancer database was reviewed retrospectively for GI cancers (esophagus, stomach, liver, pancreas, colorectal, and hepato-pancreato-biliary) from 2007-2017. Logistic regression was used to adjust for cofounders. Kaplan-Meier survival curves were compared using log-rank test.
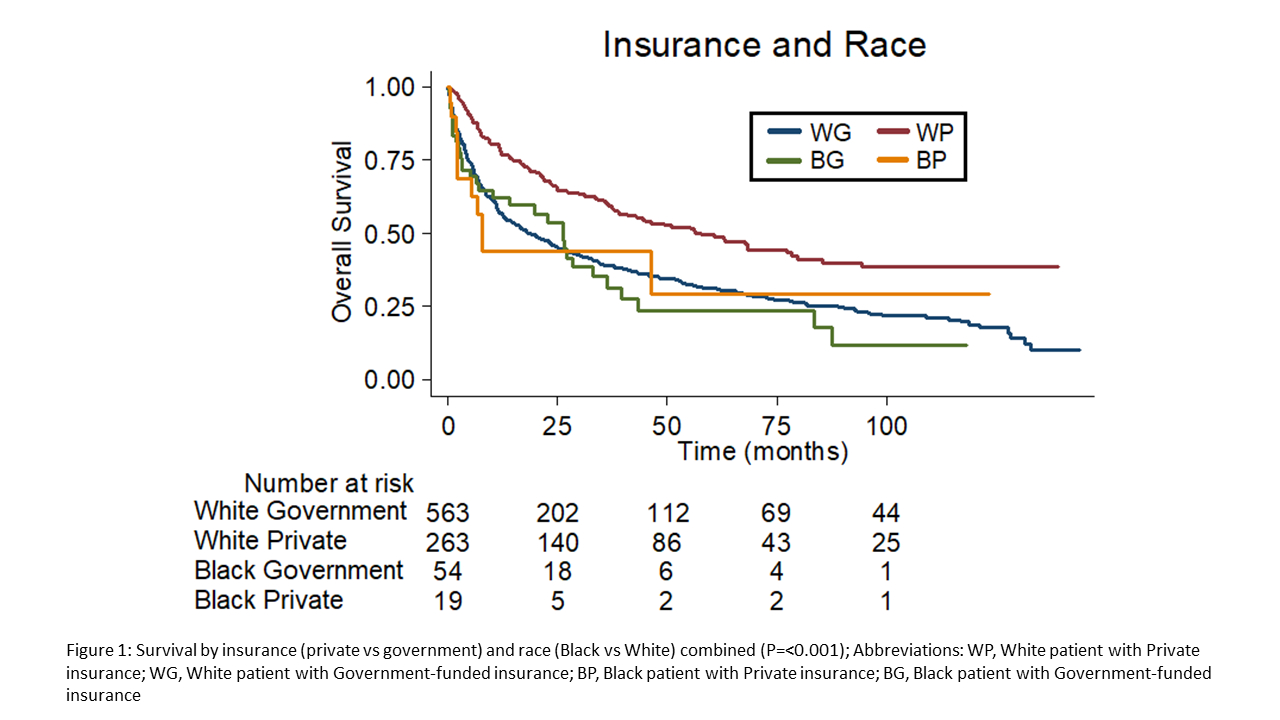
RESULTS: 1072 patients were identified. Survival improved in patients with private insurance compared to government-funded options [Median overall survival (mOS) 57.8 vs 21.2 months; P<.001]. Private insurance also correlated with earlier stage at diagnosis [Stage I-II= 50.9% vs 37.5%, Stage III-IV= 37.7% vs 49.1%, P<.001], increased chemotherapy use [44.2% vs 37.1%, P<.001], and more surgical intervention [62.4% vs 48.8%, P<.001]. Outcomes were inferior for Black Americans, including trend towards lower rate of surgical treatment [42% vs 54%, P=.058] and worse survival in private insurance carriers [mOS 7.8 vs 57.8 months, P=.021] and those with early stage disease [mOS 39.2 vs 81.5 months, P=.045] compared to White counterparts.
CONCLUSIONS: Insurance status has the strongest impact on the quality of GI oncologic care with negative synergistic negative effect of race for Black Americans. While governmental programs aim to improve equality of care, there remains significant disparity compared to private insurance. Moreover, private insurance doesn't correct disparity for Black Americans, suggesting the need to address structural bias.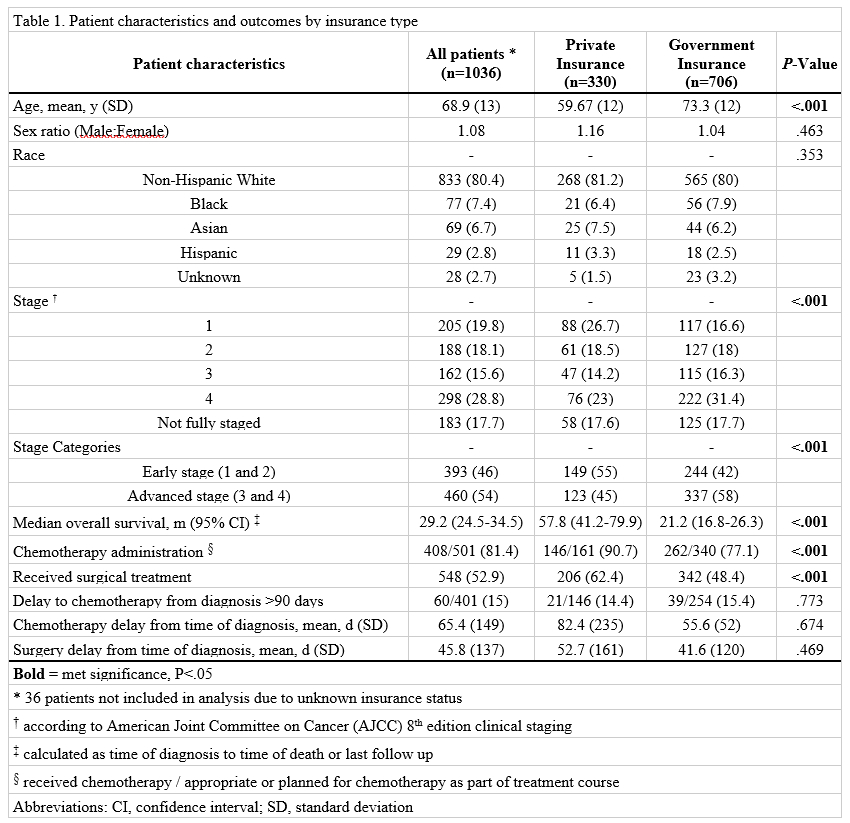
Back to 2021 Abstracts