
TRENDS IN ACHIEVING OPTIMAL OUTCOMES FOLLOWING COMPLEX GASTROINTESTINAL SURGERY: ARE PATIENTS MORE LIKELY TO ACHIEVE A TEXTBOOK OUTCOME OVER TIME?
Madison Hyer, Diamantis Tsilimigras, Adrian Diaz, Jordan Cloyd, Aslam Ejaz, Rayyan S. Mirdad, Djhenne Dalmacy, Timothy M. Pawlik*
Surgery, The Ohio State Wexner Medical Center, Columbus, OH
Background: Limited evidence exists as to how indications and outcomes among cancer patients undergoing complex gastrointestinal surgery have impacted outcomes over time. Recently, the use of composite quality measures such as "textbook outcome" has been proposed as potentially superior to individual outcomes. We sought to examine changes in the rates of "optimal" textbook outcomes among patients undergoing resection of pancreatic, liver, or colon cancer.
Methods: Medicare beneficiaries who pancreatic, liver or colon resection for a malignant indication between 2004-2016 were identified using SEER-Medicare. Rates of textbook outcomes (i.e., no complication/extended length of stay/90-day morality/90-day readmission) were assessed over time. Factors associated with achieving textbook outcomes were examined.
Results: Among 94,329 patients, 6,765 (7.2%), 1,985 (2.1%), and 85,579 (90.7%) individuals underwent resection for primary pancreatic, hepatic, or colon cancer, respectively. Over time, median patient age (median age: 2004-2007, 77 yrs vs. 2008-2011, 77 yrs vs. 2012-2016, 75 yrs) and comorbidities (median Charlson Comorbidity Index: 2004-2007, 2 vs. 2008-2011, 2 vs. 2012-2016, 2) remained similar. Overall, a total of 53,464 (56.7%) patients achieved a textbook outcome; achievement of textbook outcome varied by procedure (pancreatectomy: 48.1% vs. hepatectomy: 55.2% vs. colectomy: 57.4%, p<0.001). Of note, the proportion of patients achieving a textbook outcome increased over time (2004-2007, 53.3% vs. 2008-2011, 56.5% vs. 2012-2016, 60.1%)(5-year increase: OR 1.16 95%CI 1.13-1.18)(ptrend<0.001). The improvement in TO over time was noted for all three surgical procedures (pancreatectomy: ptrend<0.001 vs. hepatectomy: ptrend=0.02 vs. colectomy: ptrend<0.001)(Figure). Achieving a TO was independently associated with marked decreased hazards of death among all procedure types (HR 0.44, 95%CI 0.43-0.45).
Conclusion: Roughly 1 in 2 patients undergoing complex gastrointestinal surgery for a malignant indication achieved a textbook outcome. The chance of a textbook outcome following pancreatic, liver, and colon resection increased over time with textbook outcomes being associated with better long-term outcomes.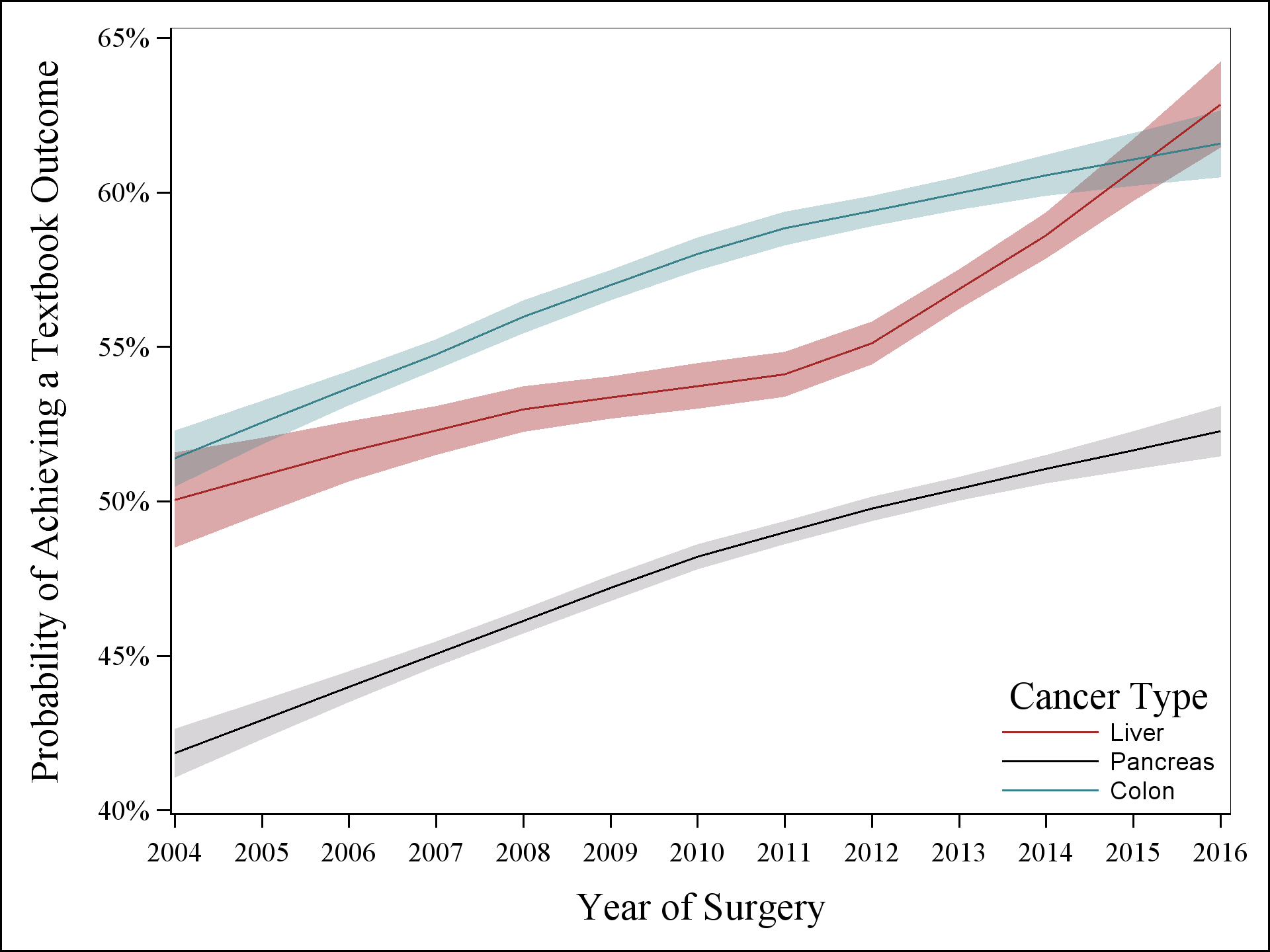
Back to 2021 Abstracts