
UNDERSTANDING THE CENTRALIZATION OF INFLAMMATORY BOWEL DISEASE HOSPITALIZATIONS AND OPERATIONS IN WASHINGTON STATE
Celine Soriano*1, Michael V. Chiorean1, Jennifer A. Kaplan1, Danielle La Selva2, James D. Lord1,2, Ravi Moonka1, Timothy L. Zisman1, Vlad V. Simianu1
1Virginia Mason Medical Center, Seattle, WA; 2Benaroya Research Institute at Virginia Mason, Seattle, WA
Background: Treatment for inflammatory bowel disease (IBD) often requires specialized care. While much of IBD care has shifted to the outpatient setting, hospitalizations remain a major site of healthcare utilization. We aimed to describe patterns of hospitalizations for IBD in Washington state (WA) to better understand variation in acuity and surgical care.
Methods: A retrospective cohort was created to include all hospitalizations captured in the WA Comprehensive Hospital Abstract Reporting System database from 2008 to 2019 for a diagnosis of Crohn's disease (CD) or ulcerative colitis (UC) using ICD-9 and ICD-10 diagnostic and procedure codes. Outpatient care or emergency department visits are not available in this database unless a hospitalization occurred. Hospitalizations were characterized by acuity (emergent vs elective) and if a procedure was performed (surgical, endoscopic, or none). Emergent and elective care was defined by acuity of admission status with "emergent" defined as requiring immediate intervention on admission. Distribution of hospitalization acuity and variation in proportion of hospitalizations resulting in procedures were analyzed over time.
Results: Over 12 years, 20,464 IBD-related hospitalizations occurred at 95 hospitals: 13,585 (66.3%) with CD and 6,909 (33.7%) with UC. There were more hospitalizations in younger patients with CD (47.3% 18-39 years, 38.6% 40-64 years, 14.1% 65 and older) than with UC (40.4% 18-39 years, 37.7% 40-64 years, 21.9% 65 and older). Emergencies represented 78.2% (n=16,024) of all IBD-related hospitalizations and did not differ between CD (78.3%) and UC (77.9%), p=0.54. Emergent hospitalizations for IBD were broadly distributed across WA hospitals (Figure 1). Surgery was performed during 10.3% (n=1,656) and endoscopy during 30.6% (n=4,895) of emergent hospitalizations. Twenty hospitals accounted for 78.3% (n= 1,299) of emergency surgeries. Elective hospitalizations were centralized (Figure 2). Operations were performed during 78.5% of elective hospitalizations, and five hospitals performed 69% of all elective surgery. Non-surgical elective admissions decreased from 35% in 2008 to 8% in 2019 (p<0.001). Laparoscopic approaches increased in both emergent (17% to 52%, p<0.001) and elective operations (18% to 42%, p<0.001) during this time period.
Conclusion: In WA, fewer than one in four hospitalizations for IBD were elective, and the vast majority were related to surgery. Emergent care is decentralized and infrequently associated with surgery. Accordingly, emergent operations are widely dispersed while elective operations are predominantly centralized at a few high-volume centers. Understanding the distribution in utilization of hospitalizations and operations for IBD patients can guide treatment decision-making and lead to standardization of emergent medical and elective surgical care.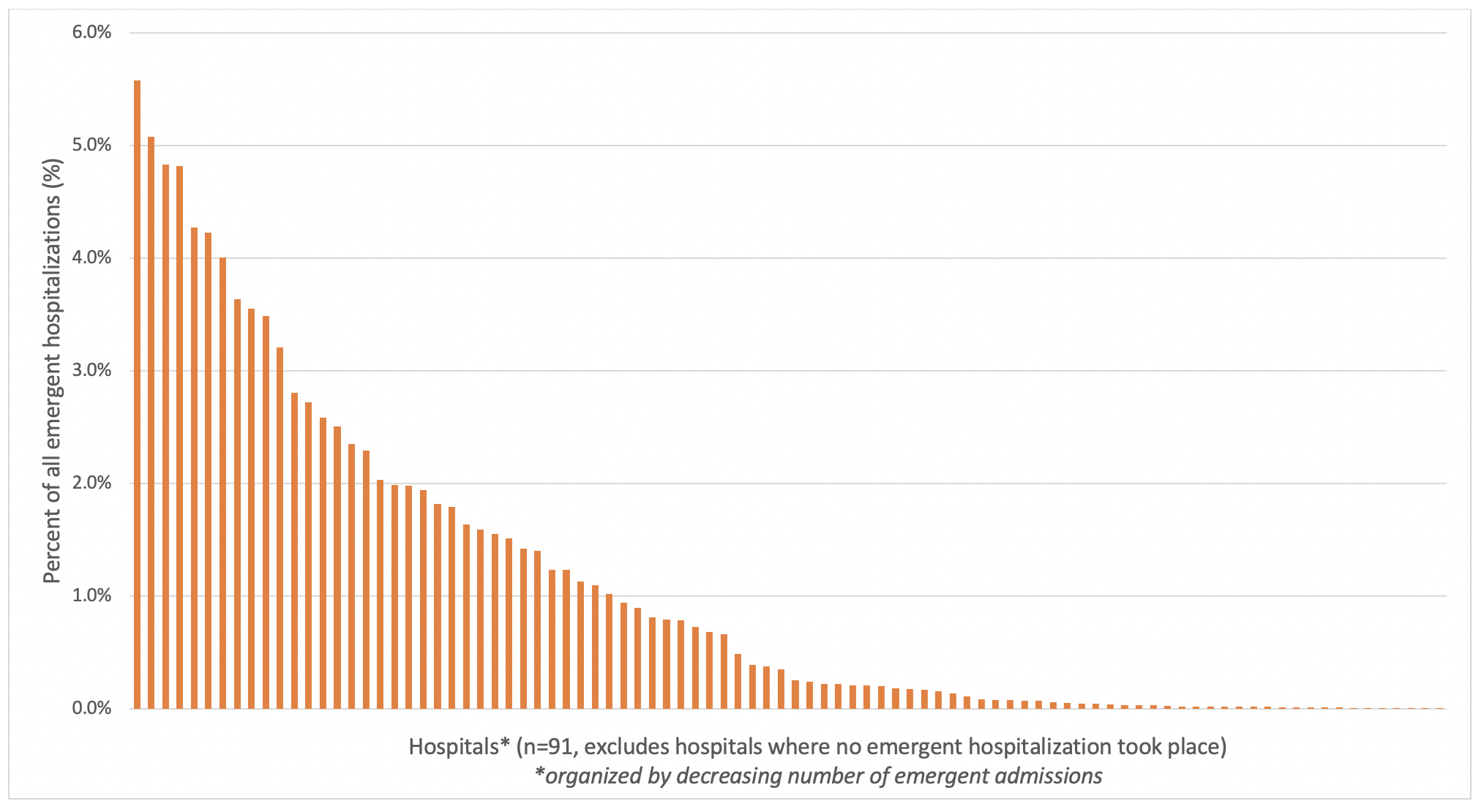
Figure 1: Distribution of emergent hospitalizations for IBD by hospital in Washington state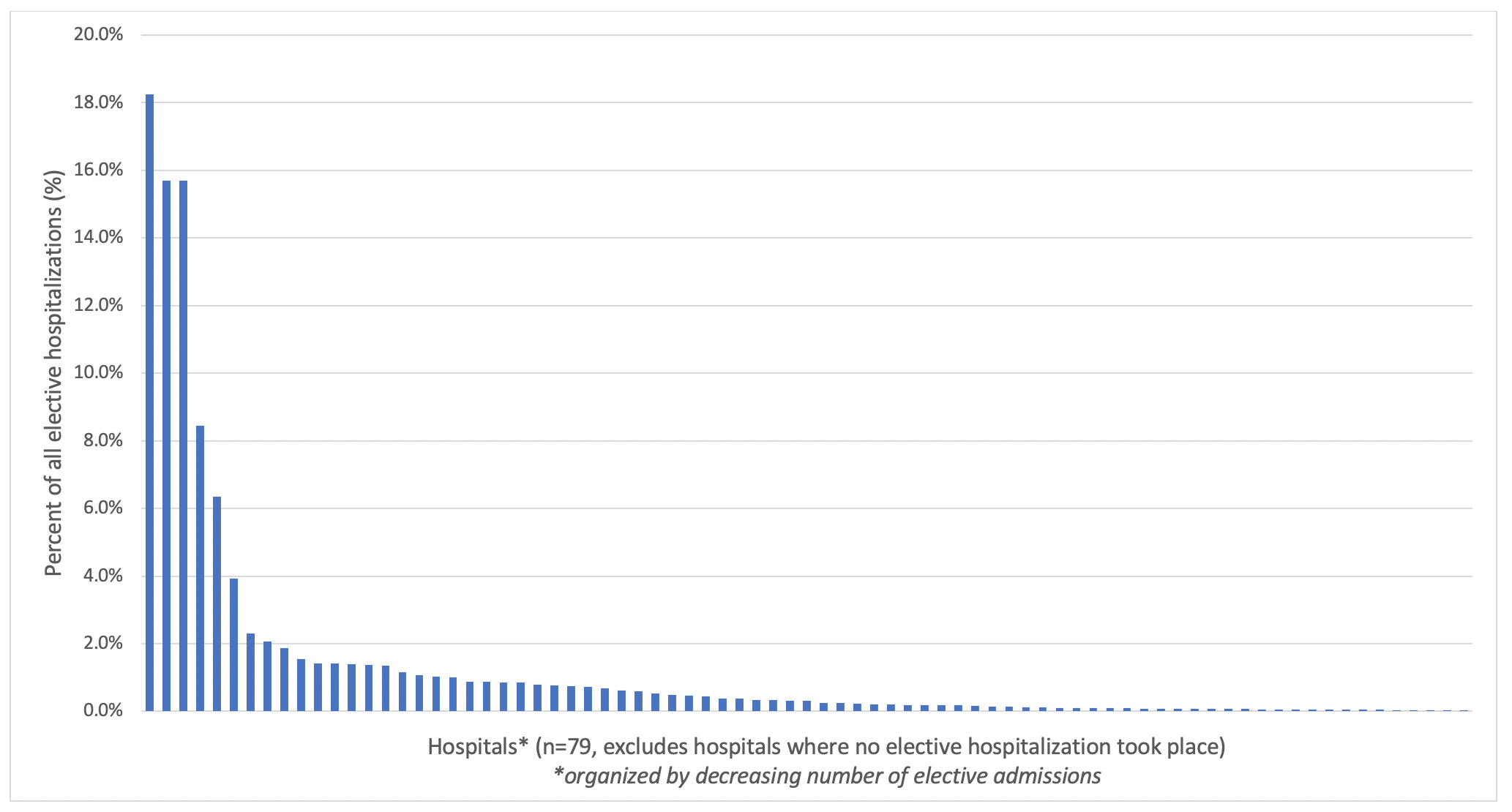
Figure 2: Distribution of elective hospitalizations for IBD by hospital in Washington state
Back to 2021 Abstracts