
OUTCOMES OF SEGMENTAL RESECTION FOR INFLAMMATORY BOWEL DISEASE-ASSOCIATED COLORECTAL CANCER
Jessica A. Holland*1,2, Tharani Anpalagan3, Mai Iwaya4, James Conner2, Anthony De Buck2, Mantaj S. Brar2
1General Surgery, McGill University, Montreal, QC, Canada; 2University of Toronto Faculty of Medicine, Toronto, ON, Canada; 3Western University, London, ON, Canada; 4Shinshu Daigaku Daigakuin Igakukei Kenkyuka Igakubu, Matsumoto, Nagano, Japan
Background:
The current standard of care for the treatment of inflammatory bowel disease (IBD)-associated colorectal cancer (CRC) or high-grade dysplasia is a total proctocolectomy. However, this practice is based on relatively low-quality evidence. The risk of metachronous colorectal cancer and the oncological outcomes of patients undergoing segmental colectomy are poorly reported.
Methods
We conducted a retrospective review of patients with IBD-associated CRC at a single high-volume IBD centre between 2000-2018. We selected patients who underwent segmental resection for the treatment of CRC. We performed a planned subgroup analysis of patients who did not undergo a planned completion proctocolectomy following their cancer surgery. The primary outcomes of interest were the rate of metachronous CRC and luminal recurrence during follow-up and their oncological outcomes.
Results
Forty-two patients met our inclusion criteria. Thirty (71%) of patients were diagnosed pre-operatively with CRC, and synchronous cancers were found in 4 (10%) on resection. The median age was 52, and most had a long duration of IBD prior to their resection (median 25y). Median follow-up was 25 mo. Of the 32 patients who did not undergo subsequent extended resection, no patients were diagnosed with a metachronous CRC (95% CI 0, 8%) and two patients (6%) were diagnosed with a luminal recurrence (95% CI 1%, 20%). The overall survival at 5 years was 69% (95% CI 48%, 83%) and disease-free survival was 57% (95% CI 37%, 72%). IBD phenotype was not associated with outcomes (unadjusted and adjusting for stage).
Conclusion
Segmental resection for IBD-associated CRC was not associated with a high risk of metachronous cancer or luminal recurrence. Overall oncological outcomes were poor suggesting that the initial CRC prognosis may overshadow the risk of metachronous cancer. Further work is required to identity patients for whom segmental resection may be appropriate, as well as factors that determine patient preference for the type of surgical resection in this setting.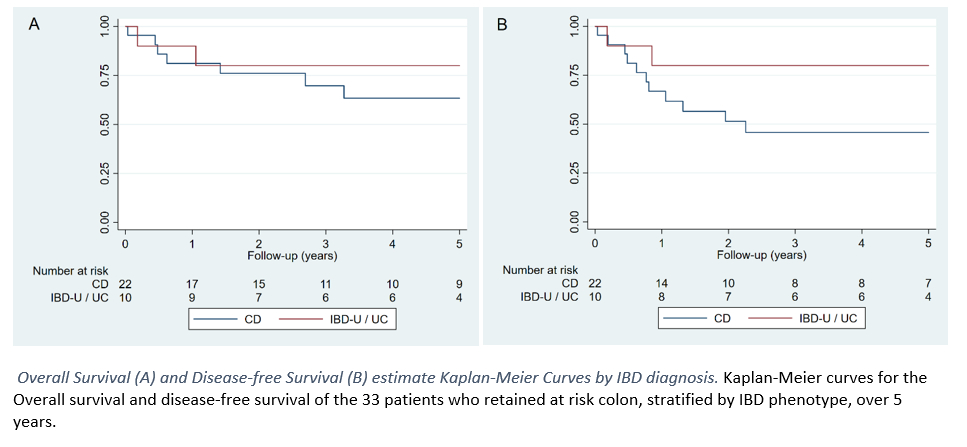
Back to 2021 Abstracts