
VENOUS THROMBOEMBOLISM DURING INDEX ADMISSION FOR ROUX-EN-Y GASTRIC BYPASS INCREASES ONE YEAR MORTALITY
Jessica X. Yu*1, Marwan S. Abougergi2,3, Allison R. Schulman1
1Gastroenterology, University of Michigan, Ann Arbor, MI; 2Internal Medicine, Division of Gastroenterology, University of South Carolina Medical School, Columbia, SC; 3Catalyst Medical Consulting, Simpsonville, SC
Background: Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE), during index admission is among the most feared complication following Roux-en-Y gastric bypass (RYGB), and is a well-documented risk factor for 30-day mortality. Little is known about the long-term risk of development of VTE and outcomes in patients who survive index admission.
Aims: To determine (1) the rate of VTE in patients with RYGB within the first year following index admission and (2) the mortality, length of stay (LOS), and healthcare utilization during this time period.
Methods: This is a retrospective cohort study using the National Readmission Database, the largest readmission database in the United States. Patients were included if they underwent RYGB during the index hospitalization during the month of January 2016. Patients were excluded if they were younger than 18 years of age. The follow-up period was 11 months. The primary outcome was the rate of VTE (DVT or PE) during the index hospitalization and the 11-month follow-up period. The secondary outcomes were: 1) in-hospital and one-year mortality after VTE 2) in-hospital and one-year resource utilization (length of stay (LOS) and total hospitalization costs and charges. Confounders were adjusted for using multivariate regression analysis and were: age, sex, Charlson comorbidity score, the median income in the patient's zip code, urban location and size.
Results: Our cohort consisted of 5,098 subjects: 1,029 with an open RYGB and 4,069 with a laparoscopic RYGB. Demographic information from index admission is shown in Table 1. The rate of VTE during index hospitalization was 6.6% and 0.4% in open and laparoscopic RYGB, respectively. The rate of VTE over 11 months after the initial admission was 1.3% and 0.5% in open and laparoscopic RYGB, respectively. Adjusted odds ratios and adjusted mean differences of outcomes are shown in Table 2. VTE during index admission was an independent risk factor for in-hospital and one-year mortality after laparoscopic RYGB (aOR 7.2, 95% CI 1.2-42.7). Index VTE was also associated with increased LOS and cost regardless of surgery subtype. VTE development following index admission was not associated with increased mortality or LOS.
Conclusions: The rate of VTE remains high following RYGB and is highest during the index admission. VTE development during the index admission carries a high long-term mortality. However, delayed development of VTE is low and not a risk factor for death at one year. Continued emphasis on VTE prevention and treatment during the index admission is crucial for improved long-term outcomes following RYGB.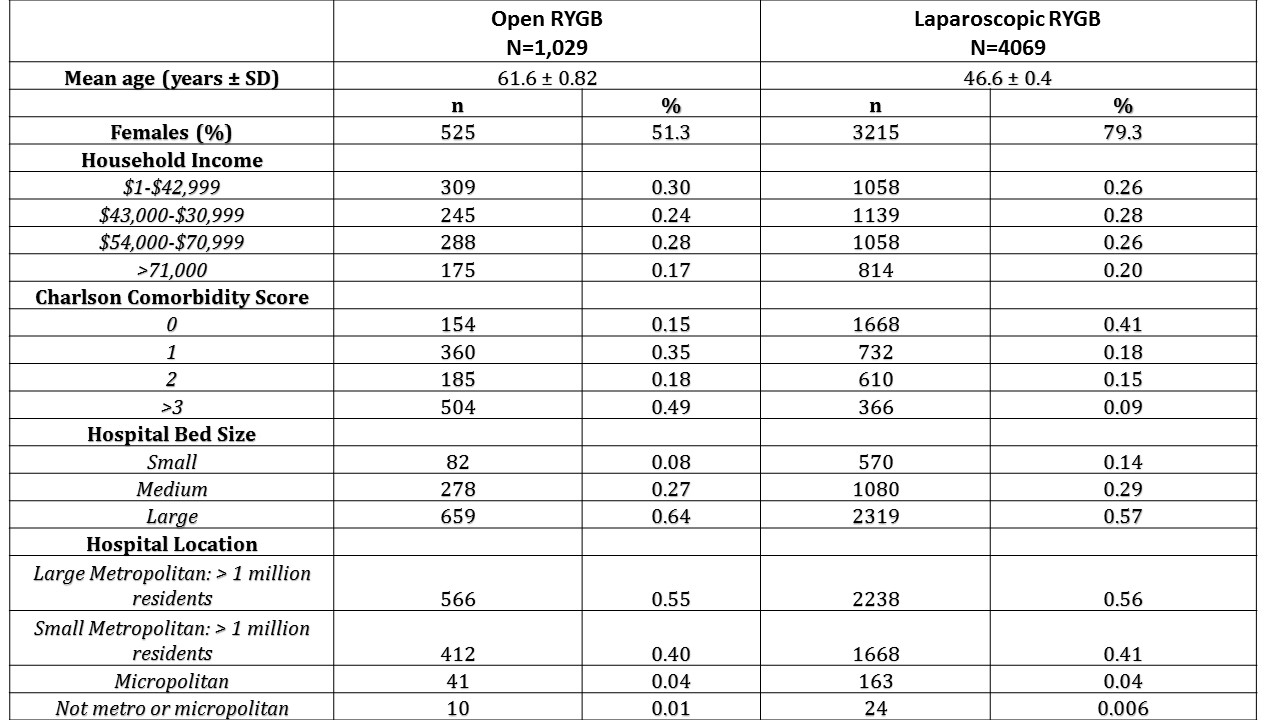
Table 1. Outcomes after bariatric surgery, index hospitalization versus 11 months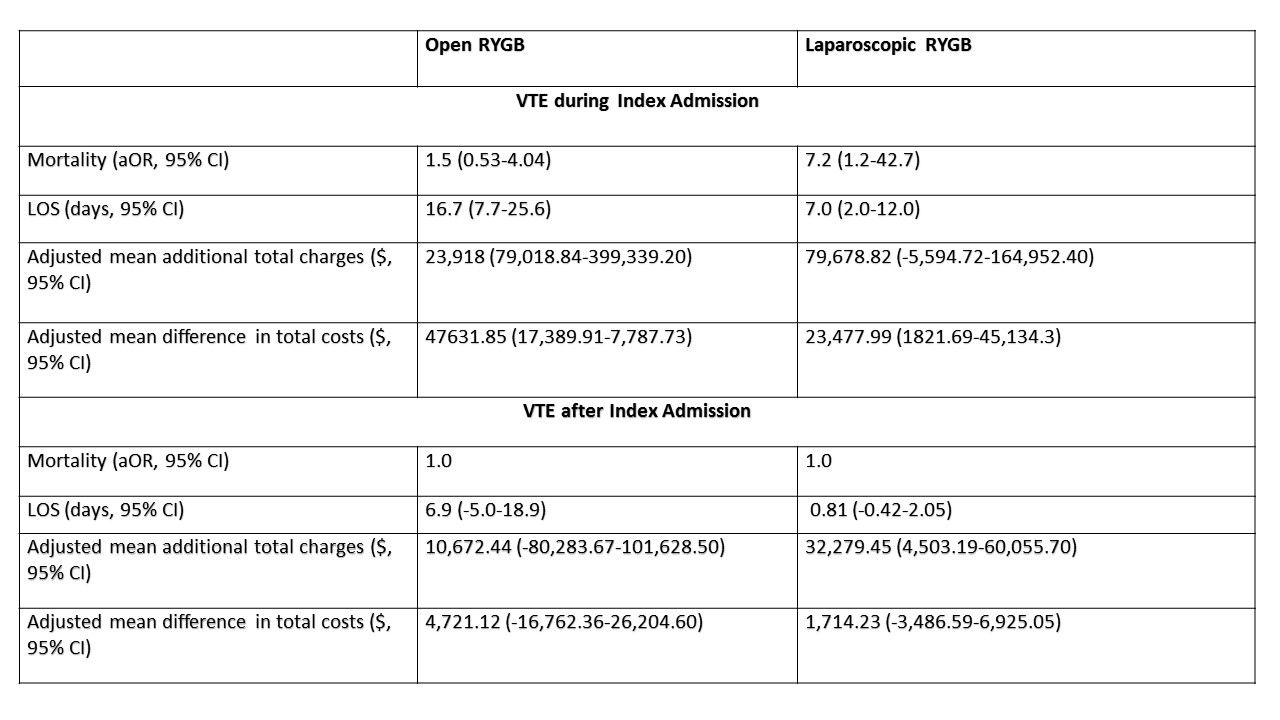
Table 2. Results of multivariate analysis based on VTE versus no VTE during index admission.
Back to 2019 Posters



