
CHASING ZERO CUFF: ROBOTIC DISTAL DISSECTION SUPERIOR TO LAPAROSCOPY IN ILEAL POUCH ANAL ANASTOMOSIS
Alexandra W. Elias*1, Ron G. Landmann2
1Surgery, Mayo Clinic, Jax Beach, FL; 2Colon and Rectal Surgery, Baptist MD Anderson Cancer Center, Jacksonville, FL
Introduction: Improved rectal dissection allows more distal transection and minimization of the rectal cuff during pouch procedures. Data is limited comparing robotic versus laparoscopic ileal J pouch-anal anastomosis (IPAA) procedures. Herein, we sought to compare robotic versus laparoscopic ileal pouch-anal anastomosis outcomes.
Methods: A prospectively maintained database was utilized to perform a retrospective matched cohort study. 44 consecutive patients who underwent ileal pouch-anal anastomosis between 2008-2017 at a US tertiary care hospital via robotic approach were matched to 72 laparoscopic controls by surgeon, age, gender, BMI, comorbidities, and operative history. Distal extent of dissection, intraoperative, and postoperative outcomes were analyzed.
Results: 116 patients (58% male) with median age 37.8 years [range 1716-68], BMI 24.5 [range 16.1-40.7], ASA score II [range I-III] underwent restorative ileal pouch-anal anastomosis (44 robotic, 72 laparoscopic), predominantly (90%) for ulcerative colitis. Distal extent of dissection (distance from dentate line) was significantly improved robotically (0 versus 1.3cm) (p<0.001). There were no significant differences in blood loss, complications, number of bowel movements at 30-days, 1 and 2 years, or use of pre-operative immunomodulators, steroids, ASA-derivatives, or TPN; however, more robotic patients utilized biologics (p = 0.007). Robotic procedure length was 20 minutes longer. Robotic median time to diet resumption was shorter (1 versus 2 days) (p<0.001). Despite equal medians, robotic admission length (4 days) and time until ostomy function (1 day) was significantly shorter (p = 0.02 and p=0.005, respectively). There were no reoperations or mortalities.
Conclusion: Robotic surgery enables superior total mesorectal excision and distal transection with elimination of the at-risk rectal cuff with improved postoperative outcomes in patients undergoing IPAA for ulcerative colitis and familial adenomatous polyposis. This technique can be applied to inflammatory and oncologic operations to improve negative margin rates and improve rates of sphincter preservation/intestinal continuity.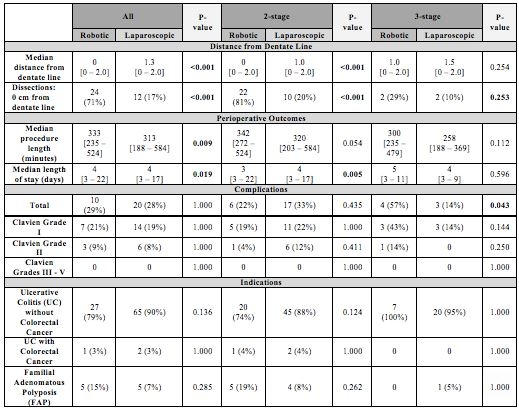
Back to 2019 Posters



