
ENDOSCOPIC ASSISTED LAPAROSCOPIC REPAIR OF DISTAL ESOPHAGEAL PERFORATION IN BOERHAAVE'S SYNDROME
Bernardo M. Pessoa*, Matthew G. Browning, Jad Khoraki, Gretchen Aquilina, Jennifer Salluzzo, Guilherme Campos
VCU, Richmond, VA
IMPORTANCE: Emergent surgical repair of distal esophageal perforations is preferred in most, however reported peri-operative morbidity is high and laparoscopic surgery is seldom used. We report two patients with distal esophageal perforation in Boerhaave's syndrome that were repaired laparoscopically assisted by endoscopic localization, and present a review of the literature.
OBJECTIVE: Discuss the option of laparoscopic surgery, endoscopically assisted, to treat distal esophageal perforations in Boerhaave's Syndrome.
METHODS: Retrospective review of outcomes of two consecutive cases in which laparoscopic surgery was used to treat an esophageal perforation and present a systematic literature review.
RESULTS:
Patient 1: A 22 y/o male was evaluated at outside facility with chest pain after choking with food and vomiting. An endoscopy confirmed diagnosis of perforation; patient was intubated and transferred to our facility 7 hours after symptoms started. At admission, a CAP CT showed extensive pneumomediastinum.
Patient 2: A 55 y/o male presented to an outside facility with chest pain after choking with food and vomiting. CT scan showed pneumomediastinum and patient was transferred to our hospital. An UGI confirmed the diagnosis.
Both patients were taken to the OR for a laparoscopic exploration and endoscopic assisted repair.
Operative Report: At laparoscopy, the GE junction and distal esophagus were mobilized using standard laparoscopic techniques and upper endoscopy assisted localizing the perforations (Picture 1). Patients 1 had a perforation extending for 4 cm above the GE junction (Picture 2); Patient 2 had a 2 cm long perforation starting 4 cm above the GE junction. After esophagus was circumferentially dissected, the esophageal mucosal disruption was repaired with interrupted 3-0 PDS sutures under endoscopic visualization, and esophageal muscle approximated. In both cases, the hiatus was closed and a Toupet fundoplication covered the repair. Both patients had complications: Patient 1 needed thoracoscopic evacuation of a hemothorax on POD 0 related to chest wall bleed from a chest tube inserted at OSH and Patient 2 developed ARDS and Acute Kidney Injury; both patients had a full recovery. Discharges were on POD 8 and 15. Both remain asymptomatic at 18 and 7 mo post-op. Repeated endoscopy showed intact esophageal mucosa and fundoplication.
Literature Review: Eight articles reported on 10 patients a laparoscopic and/or thoracoscopic repair of esophageal perforations. 9 patients had successful repairs and 1 died. The repairs were single layer suture (6) or two layer suture (4). Surgery occurred from 5 to 216 hours after admission. Perforation length range from 1-4cm. The mean discharge time was 28 days.
CONCLUSIONS AND RELEVANCE: Laparoscopic surgery, endoscopically assisted, maybe used to treat distal esophageal perforations in Boerhaave's Syndrome.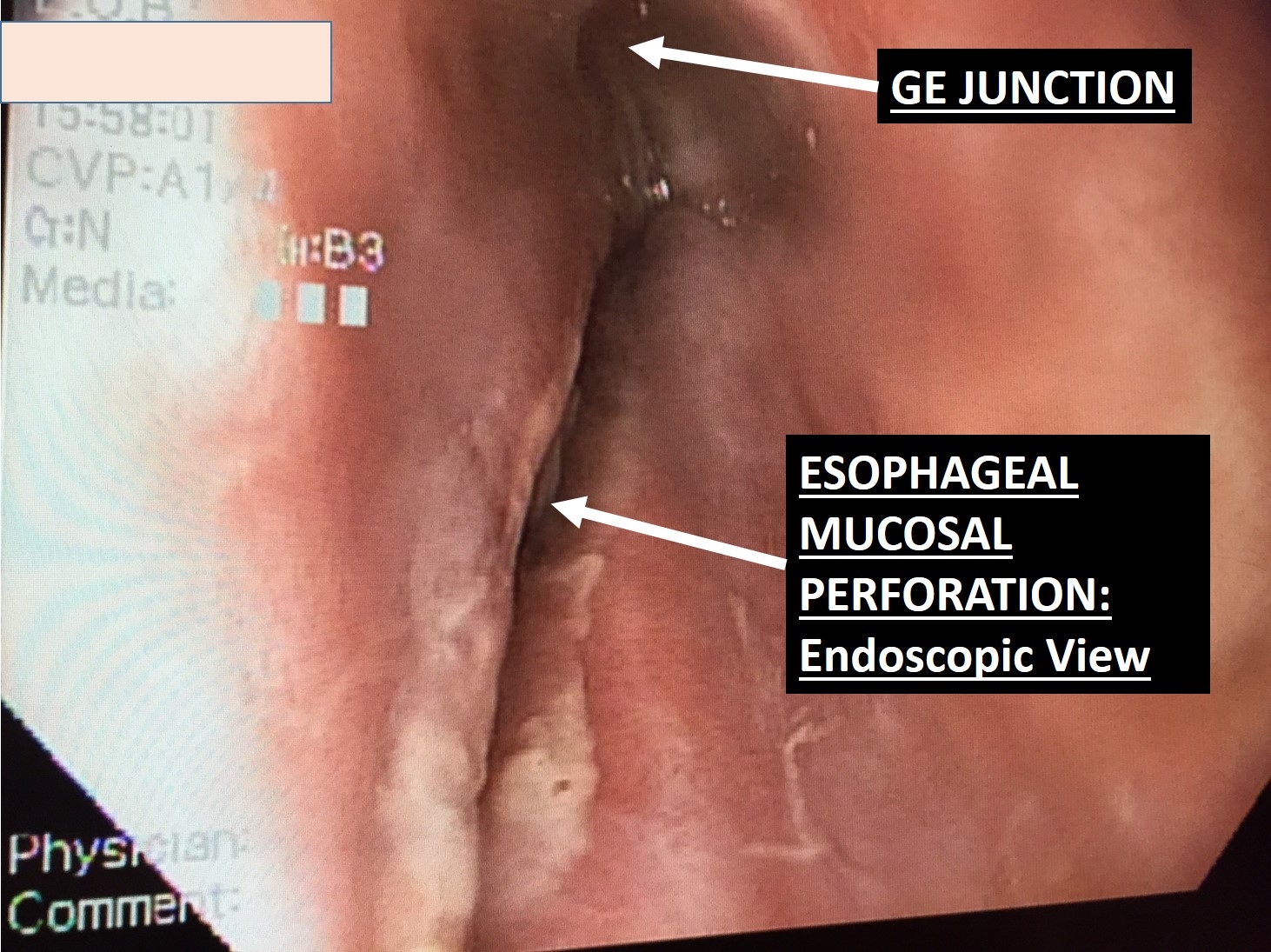
Intra-operative Endoscopic View of Distal Esophageal Perforation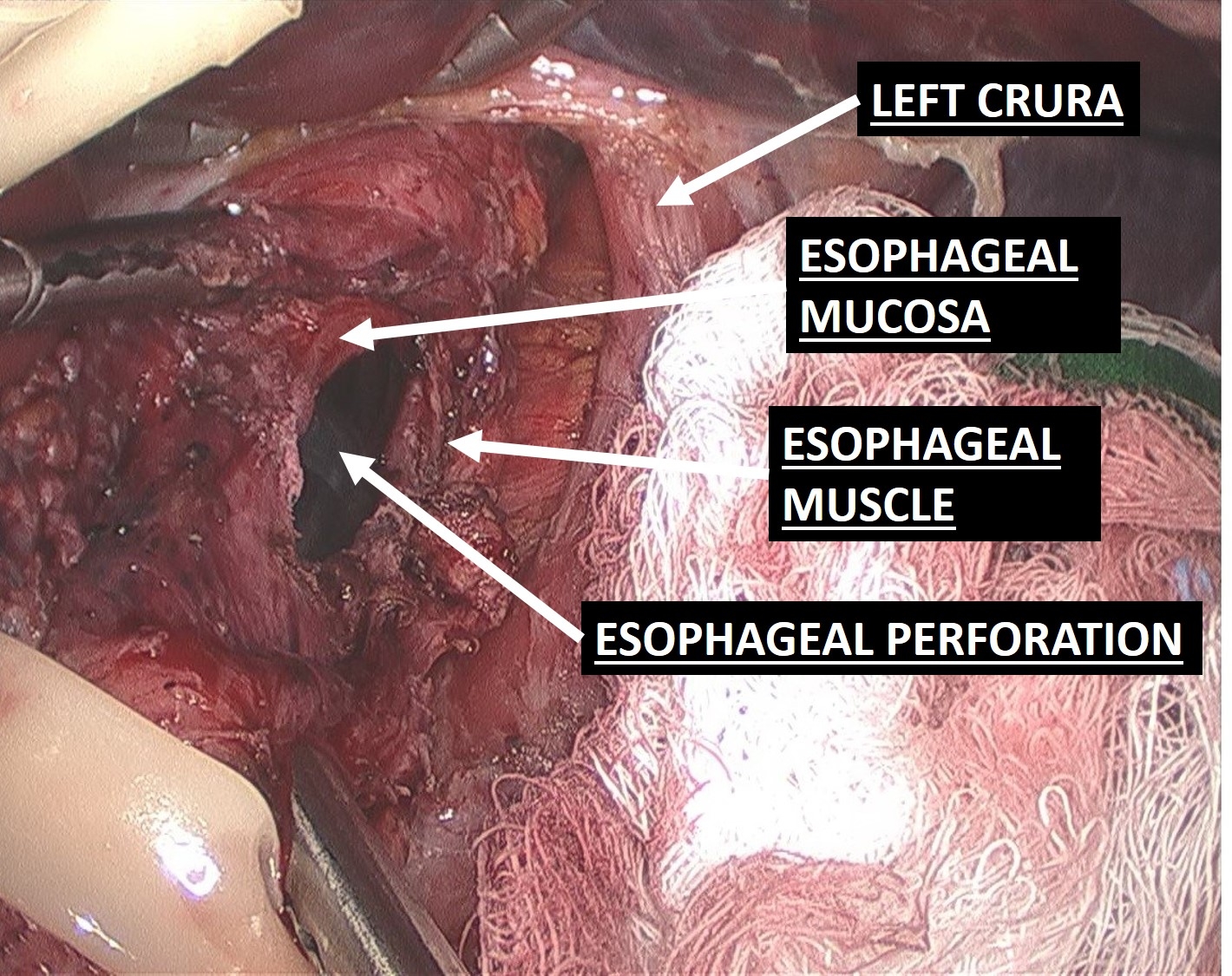
Laparoscopic View of Distal Esophageal Perforation
Back to 2019 Posters



