
WHAT DEFINES CLINICALLY SIGNIFICANT WEIGHT REGAIN AFTER ROUX-EN-Y GASTRIC BYPASS FOR PATIENTS WITH HYPERTENSION?
Kelly Hathorn*, Pichamol Jirapinyo, Ahmad Najdat Bazarbashi, Walter W. Chan, Christopher C. Thompson
Brigham & Women's Hospital, Boston, MA
Background: Patients who regain weight after Roux-en-Y Gastric Bypass (RYGB) are at increased risk for the development or recrudescence of comorbidities. No data-driven definition of clinically significant weight regain exists to date. Our aim is to determine the percent weight gain that significantly increases the risk of developing hypertension (HTN).
Methods: Methods: This was a retrospective cohort study conducted at a single academic institution. The Research Patient Data Registry (RPDR) was used to extract adult patients (age ≥18) who experienced weight regain following RYGB and were referred to Bariatric Endoscopy clinic between 1/2003 and 9/2018. Patient demographics, medical comorbidities, surgical history, weight trends pre- and post-operatively and excess body weight loss (EBWL, adequate defined as 50%), were reviewed. New development or worsening of pre-existing HTN was recorded after the onset of weight regain, based on presence of: diagnosis code or provider documentation of condition and/or medication initiation or anti-hypertensive dose escalation. Weight at the time of documentation of new or worsening HTN was used to determine the percentage weight regain defined as [(Weight at Visit)-(Nadir Weight)/(Pre-Bypass Weight)-(Nadir Weight)}*100. Statistical analysis was completed using Kaplan Meier analysis and Cox regression analysis
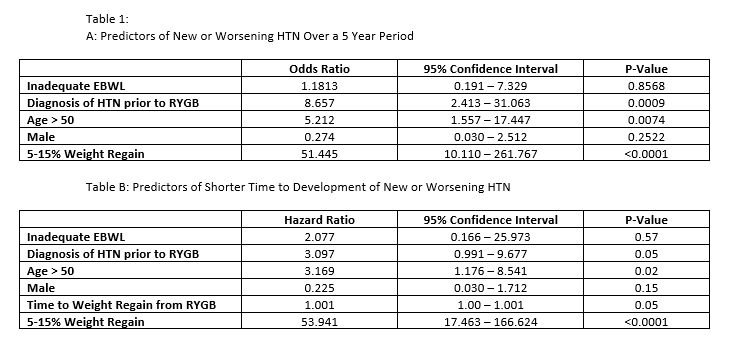
Results: 529 patients were enrolled in this study. Among those patients with 5-15% weight regain, 84% developed new or worsening HTN, compared to 6.15% of those with <5% weight regain in a 5-year period from onset of regain (p=<0.0001). Prior diagnosis of HTN, age ≥ 50, and 5-15% weight regain were independently associated with development over a 5-year period from onset of regain (p=0.0009, 0.0074, and <0.0001, respectively; Table1A). On Kaplan-Meier analysis, those with a diagnosis of HTN prior to RYGB (p=<0.001), inadequate EBWL (p=0.0006), age ≥ 50 (p=<.0001), and 5-15% weight regain (p= <0.0001; Figure 1) had a shorter time to development or worsening from onset of regain. Independent predictors were: diagnosis of HTN prior to RYGB (p=0.05), age ≥ 50 (p=0.02), time to onset of weight regain from RYGB (p=0.05) and 5-15% weight regain (p=<0.0001, Table 1B). Inadequate EBWL and gender were not predictors of shorter time to development or worsening of HTN (Table 1B).
Conclusions: Patients who regain weight after RYGB, pre-RYGB HTN, older age, and 5-15% regain were independent predictors of new or worsening HTN and predicted a shorter time to development after the onset of regain. This demonstrates that weight regain of >5% is clinically significant and independently associated with HTN. The conventional 15% cut-off for significant regain should be adjusted, and earlier intervention should occur to prevent long-term complications.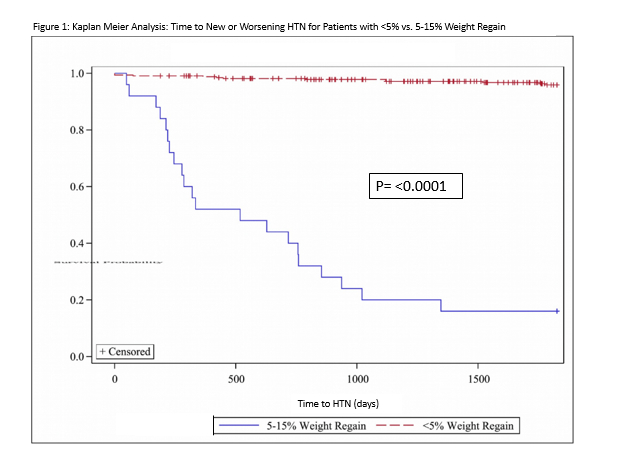
Back to 2019 Posters



