
COLECTOMY IN PATIENTS WITH TOXIC MEGACOLON: A REVIEW OF NATIONAL INPATIENT DATABASE
Mohamed Tausif Siddiqui*1, Mohammad Bilal2, Lakshmi Asritha Gollapudi3, Dhruv Mehta3, VIrendra Tewari3
1Internal medicine, New York Medical College, White Plains, NY; 2Gastroenterology and Hepatology, University of Texas Medical Branch, Galveston, TX; 3Gastroenterology & Hepatology, New York medical College, Valhalla, NY
Background
Toxic Megacolon (TM) is a life-threatening complication of bowel inflammation which can occur secondary to an infectious or non-infectious etiology. Surgical intervention is indicated in when there is progressive colonic dilation, clinical deterioration despite optimum medical therapy and peritonitis. Subtotal colectomy with end ileostomy is the surgical treatment of choice.
Aim
We aimed to assess the trends of surgical management for TM as well as its impact on outcomes.
Method
Patients hospitalized with a primary discharge diagnosis of toxic megacolon were included from the National Inpatient Sample (NIS) 2005-2014 by using disease-specific ICD 9 CM diagnostic code (ICD 9 code 55.82). Hospitalizations with age less than 18 years were excluded. The primary outcome measure was to identify the 10-year rate of surgery in patients with TM. Secondary outcomes were the impact of surgery in patients hospitalized with TM on in-hospital mortality and healthcare resource utilization.
Results:
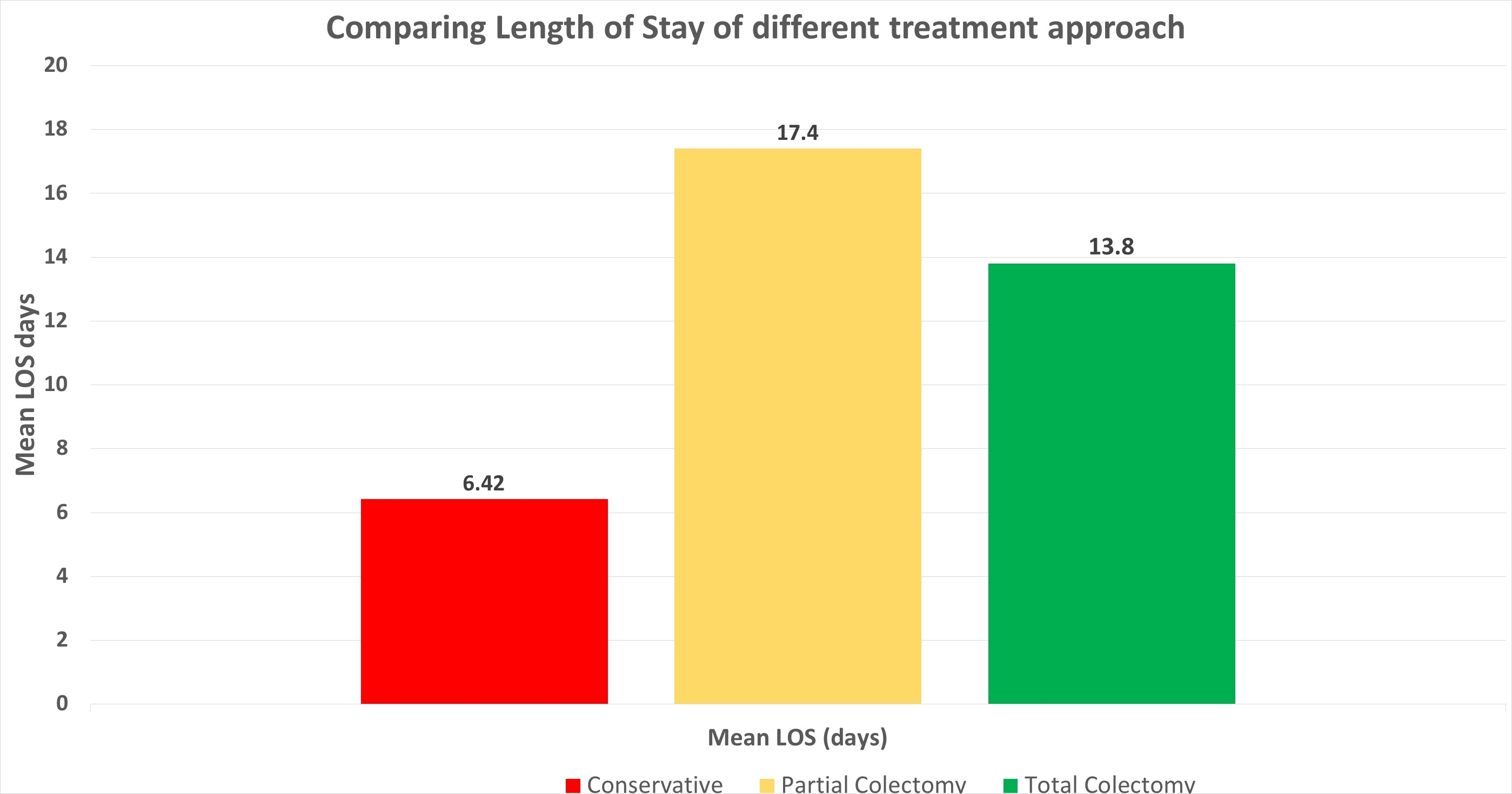
A total of 9,374 adult hospitalizations across the US with a primary diagnosis of TM were identified between the years 2005 to 2014. Out of these 297 (3.2%) patients underwent surgery. 58% (N=172) of those were partial colectomy (Laparoscopic approach N=5 & open approach N=167) & 42% (N=125) were total colectomies (Laparoscopic approach N=10 & open approach N=115). In-hospital mortality in patients who were treated conservatively was 3.2% in contrast to 18.2% in patients who underwent surgery. In-hospital mortality in patients who underwent total colectomy was lower (11%) as compared to those who underwent partial colectomy (22.4%). Mean LOS associated with conservative management ( 6.42 days), partial colectomy (17.4 days), total colectomy(13.87 days). Mean hospital cost associated with conservative management ($9934), partial colectomy ($43,989), total colectomy ($40,231). We assessed the impact of conservative versus surgical management based on the severity of illness subclass ( Fig.A )
Conclusions: Total colectomy appears to be associated with decreased in-hospital mortality as well as shorter LOS and lower cost of care in comparison to partial colectomy.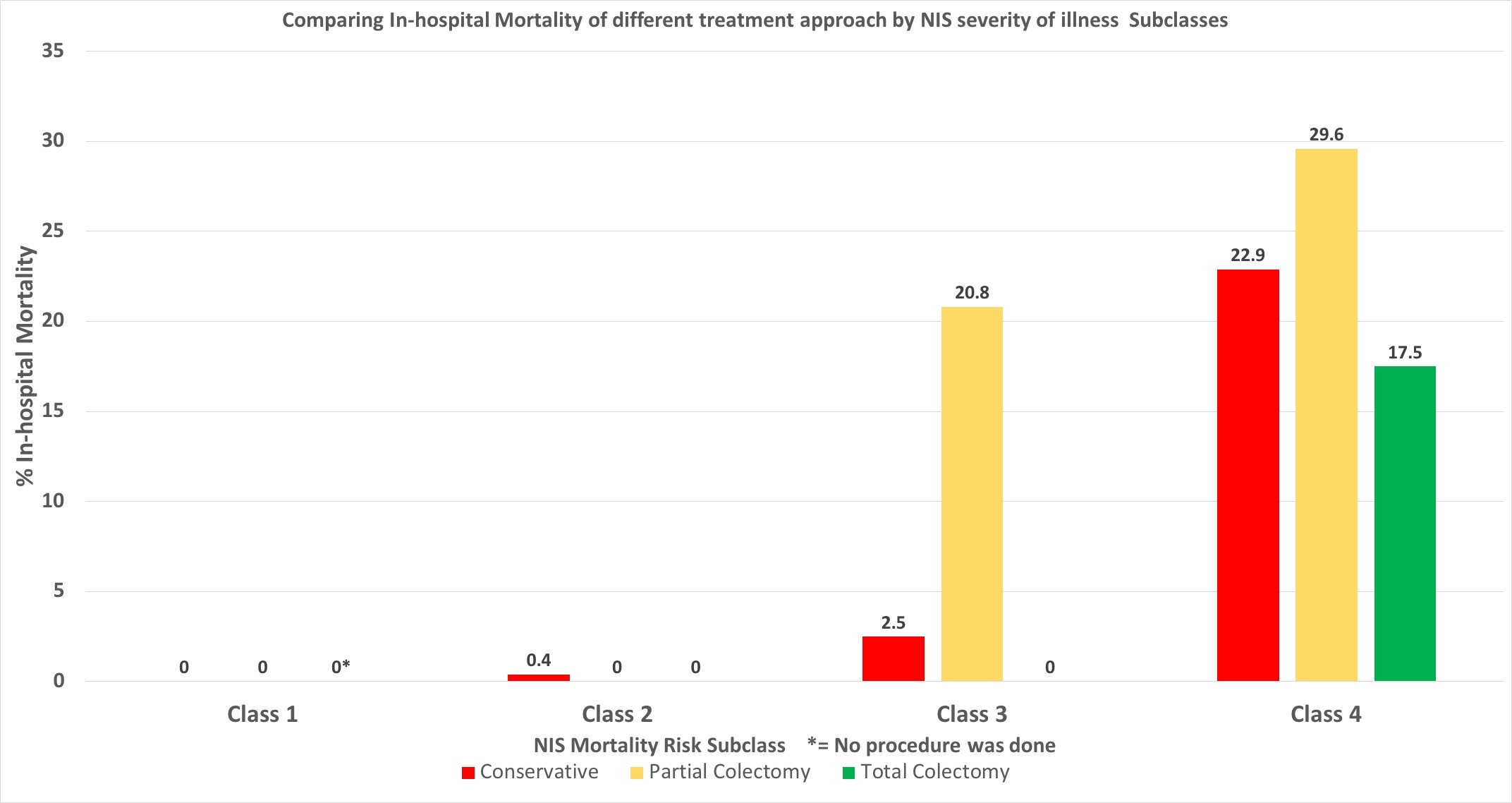
Back to 2019 Posters



