
ANAL SQUAMOUS CELL CARCINOMA: RADIATION THERAPY ALONE MUST BE AVOIDED
Jonathan Efron1, Hamda Almaazmi*1,3, James Taylor1, Miloslawa Stem1, David Yu2, Brian D. Lo1, Bashar Safar1
1Surgery, Johns Hopkins University, Baltimore, MD; 2Surgery, Queen's University School of Medicine, Kingston, ON, Canada; 3Surgery, Tawam Hospital, Al Ain, Abu Dhabi, United Arab Emirates
BACKGROUND
Anal cancer accounts for 2.7% of all gastrointestinal neoplasms in the United States. Anal squamous cell carcinoma (ASCC) is the most common histological subtype. Rates have increased in recent years, proposed to be due to high-risk sexual behavior and infectious agents such as Human Papilloma Virus, which is a known risk factor in the development of the premalignant anal intraepithelial neoplasia. Combined chemoradiaton therapy (CCRT) is the gold standard of treatment for ASCC. The aim of this study is to assess the trends in ASCC prevalence and treatment, along with overall survival (OS) by stage and treatment type.
METHODS:
Patients diagnosed with stage I - IV ASCC were identified from the National Cancer Database from 2004 to 2015. The primary outcome was 5-year OS, which was analyzed using Kaplan-Meier survival curves, log-rank test, and Cox proportional hazards models.
RESULTS:
34,613 cases were included (I: 21.45%; II: 41.00%; III: 31.62%; IV: 5.94%), with a notable increase in prevalence of stage III and IV disease (III: 4.12% in 2004 to 12.69% in 2016; IV: 4.96% to 13.18%; p<0.001 each). 87.24% of the sample had a concurrent diagnosis of anal intraepithelial neoplasia. CCRT was the most utilized treatment modality (59.47%), followed by CCRT with surgery (multimodal therapy, 22.68%), surgery alone (9.54%), radiation alone (3.40%), radiation with surgery (2.06%), and other (2.85%). Stage I patients had the best 5-year OS (I: 80.80%; II: 69.04%; III: 57.76%; IV: 23.27%; p<0.001)(Table 1). Multi-modal treatment offered the best OS rates for stage I, II and IV cancers (I: 84.87%; II: 75.12%; III: 60.34%; IV: 33.08%), and comparable survival to those treated with CCRT alone for stage III cancer (III: 61.14%) (Figure 1). Radiation alone had the worse OS rates (I: 54.20%; II: 36.23%; III: 28.72%; IV: 8.21%). On adjusted analysis, radiation treatment alone had the greatest risk of mortality (I: Hazard Ratio 2.01, 95% CI 1.14-3.54, p=0.016; II: 2.05, 1.44-2.93, p<0.001; III: 2.30, 1.98-2.67, p<0.001; IV: 1.99, 0.99-4.02, p=0.054), and there was no difference in HR between patients treated with the multi-modal treatment versus CCRT for stage I, II, and IV cancers. Patients with anal intraepithelial neoplasia had a comparable OS to those without the condition.
CONCLUSION:
ASCC has increased in prevalence, notably in stage III and IV disease. Though CCRT is the most commonly utilized treatment type for all stages of ASCC, multi-modal treatment offers better OS rates in stages I, II and IV. There is no difference in the risk of mortality between multi-modal treatment and CCRT for stages I, II, and IV. Treatment with radiation alone offers the worst OS no matter the stage, and should no longer be employed as a solitary treatment modality.
KEY WORDS:
Squamous Cell Carcinoma; Anal Cancer; Chemoradiation therapy; Radiation therapy; Survival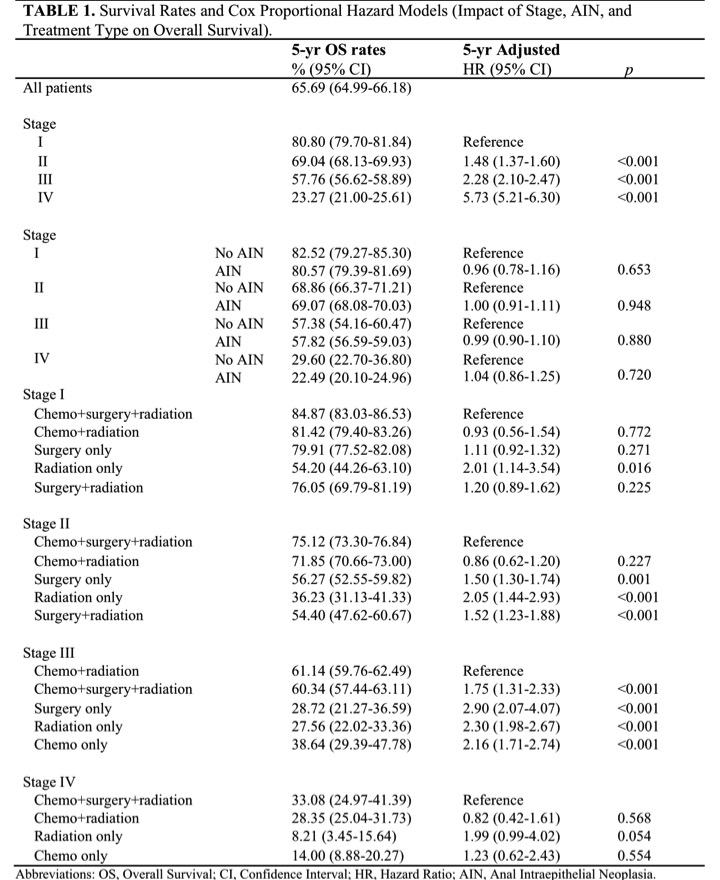
Table 1. Survival Rates and Cox Proportional Hazard Models (Impact of Stage, AIN, and Treatment Type on Overall Survival).
Figure 1. Kaplan-Meier Curves of 5-year Overall Survival Rates for Anal Squamous Cell Carcinoma Patients Stratified by Stage and Treatment Type.
Back to 2019 Posters



