
COMBINATION OF PROGRESSIVE PNEUMOPERITONEUM, BOTULINUM TOXIN A AND TRANSVERSUS ABDOMINIS MUSCLE RELEASE AS AN ADDITIONAL BENEFIT FOR SURGICAL MANAGEMENT OF COMPLEX VENTRAL HERNIA
Leopoldo E. Castañeda Martinez*1, Andrés Olivares Ronces2
1Surgery, ABC medical center, Mexico city, Mexico, Mexico; 2Medical Assistant, ABC medical center, Mexico City, Mexico
Incisional hernia is one of the long-term postoperative complications often seen after open abdominal surgery (incidence varies from 11-20%) and are associated with considerable postoperative morbidity, risk of hernia recurrence, costs, and diminished social and physical functioning. So far, there's no generally accepted definition of complex ventral hernia (CVH), so we used the parameters described by Slater et al defining CVH as a larged-sized abdominal wall hernia with a transverse diameter of 10 cm or more.
We present the management of a CVH, on a 67 y/o hispanic male with no medical history, smoker, surgical history for laparotomy on 2013 due to a perforated gastric ulcer undergoing surgery few days later for a leak requiring long stay hospitalization. The patient presented to doctor's office on August 2018, with a midline bulge and discomfort, accompanied by heaviness and constipation. Also, a symptomatic right inguinal hernia. Upon physical examination there was a large wall abdominal defect with skin changes such as thinning, extending from subxiphoid region to lower abdomen with a 15x18 cm well-defined lump protruding through the midline after valsalva maneuver, at the expenses of a non reducible hernia content; peristalsis was ausculted inside the sac. Abdominal CT Scan was made identifying the following findings:
A hernia wall defect of 158 mm (W) x 180 mm (LEN)
Hernia Sac Volume (HSV) = 916,905.6 mm3
Abdominal Cavity Volume (ACV) = 8,062,080 mm3
Volume Ratio (VR), defined as HSV/ACV = 11%
Bilateral inguinal hernia
Preoperative preparation was made with botulinum toxin type A (BTA) injections (dilution 100 U) performed 5 weeks prior to surgical procedure. Five points on either side of abdominal wall as described by Ibarra Hurtado et al. with 10 units of BT at each point (50 U per side) by ultrasonographic guidance, and catheter placement for progressive pneumoperitoneum (PPP) was performed 8 days prior to surgical procedure inducing an initial ambient air insufflation of 800 cc until 5000 cc were completed. Pregabalin 75mg/day was used before and after surgery, additionally, smoking cessation was implemented. Surgery involved bilateral transversus abdominis muscle realease (TAR), reduction of bilateral inguinal hernia sacs, closure of the posterior sheet, placement of a 30x25 medium weight polypropylene mesh underlay and tension free closure of the anterior sheet; retrorectal Jackson Patt drain was placed prior to closure.
Through the years, benefits of BTA, PPP, CST have been studied individually. Furthermore, it is well known most of the CVH cannot be closed simply by approximating the medial rectus muscles. It is for this reason that the cornerstone for CVH is the preoperative assesment and the use of techniques in conjuction can result on a synergic effect over a tension-free closure, neverthless, the data about the results still uncertain.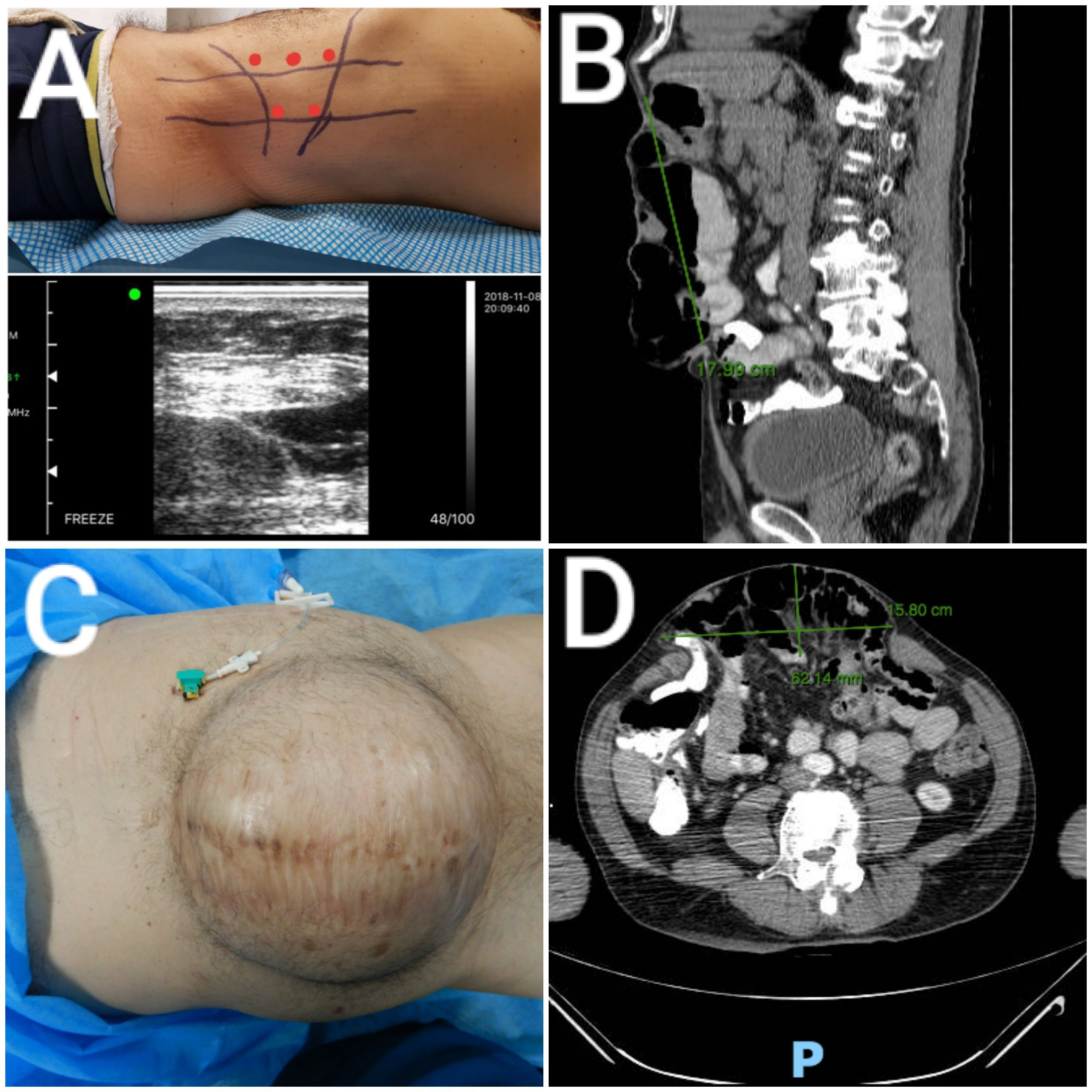
a) Representation of sites for BTA injections by ultrasonographic guidance. b) Preoperative sagital CT showing length hernia defect. c) Preoperative progressive pneumoperitoneum. d) Preoperative axial CT showing width hernia defect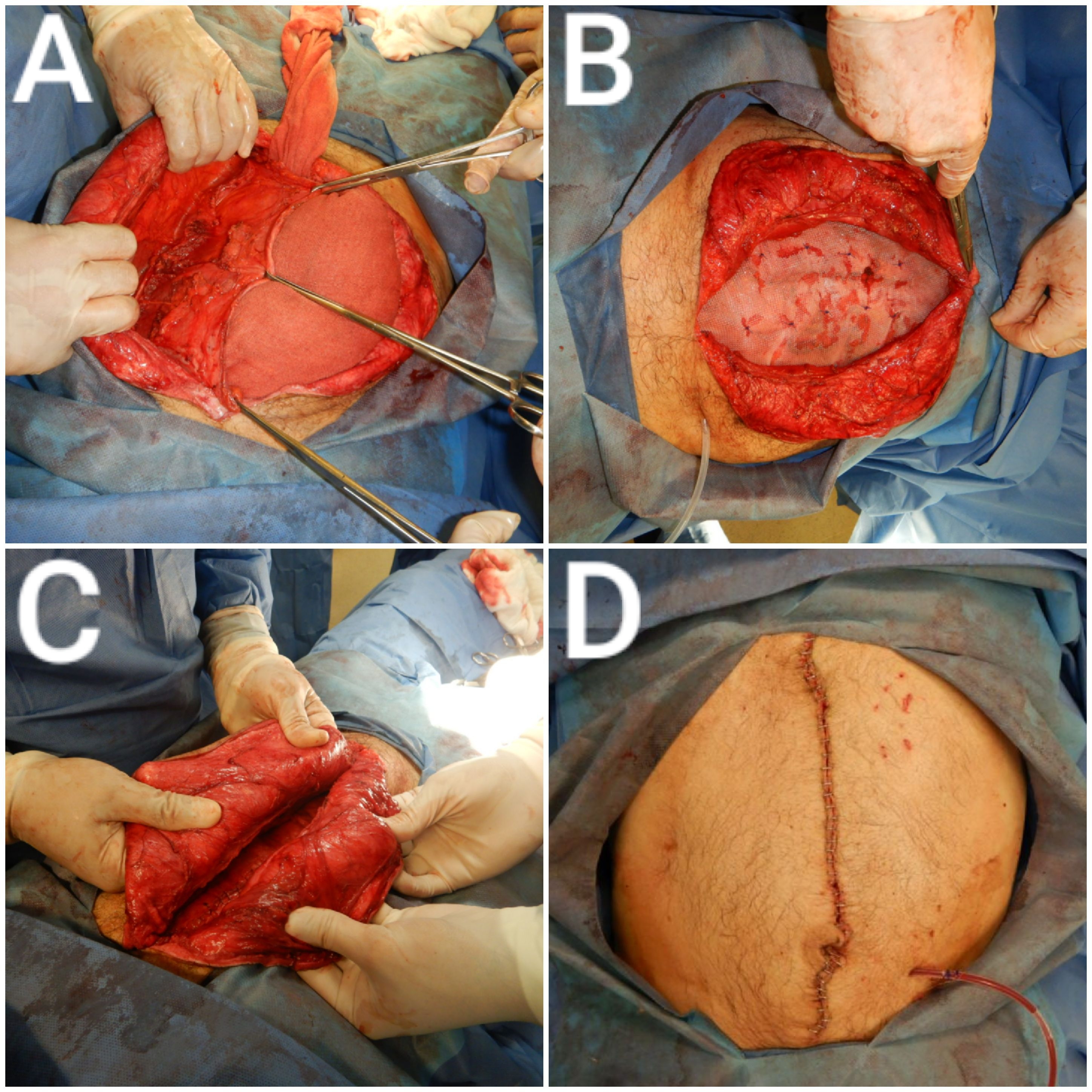
a) Transversus abdominis muscle release. b) Placement of a 30x25cm medium weight polypropylene mesh. c) Closure of the anterior sheet. d) Inmediate Postoperative with a retrorectal Jackson Pratt drain.
Back to 2019 Posters



