
PREVENTING PORT-SITE (LATERAL) HERNIAS AFTER LAPAROSCOPIC VENTRAL HERNIA REPAIR
Karla Bernardi*, Oscar A. Olavarria, Nicole B. Lyons, Puja Shah, Alexis N. Milton, Lillian S. Kao, Tien C. Ko, Mike K. Liang
General Surgery, University of Texas Health Science Center at Houston, Houston, TX
Introduction:
Lateral hernias due to port placement occur at a rate of 5% (0 - 30%) and are an under-reported complication following laparoscopic ventral hernia repair (LVHR). The majority of lateral hernias occur at previous 10-12 mm port incisions, which are often needed to safely introduce large pieces of mesh. One way to avoid using such a complication is to place the 10-12 mm port through the ventral hernia defect. However, there is theoretical concern for increased risk of surgical site infection (SSI) with this technique. We hypothesized that introducing mesh through a 10-12 mm port placed through the defect will decrease the rate of lateral hernias with no increased risk of SSI.
Methods:
This is a prospective cohort study of patients who underwent LVHR at a single academic institution from 2014-2017. All patients had mesh introduced through a 10-12 mm port placed through the ventral hernia defect. Observed outcomes were compared to expected outcomes based upon data from published systematic reviews. The primary outcome was prevalence of lateral hernias from port placement. Diagnosed by clinical exams and verified by radiographic imaging. Secondary outcomes included hernia recurrence, overall post-operative hernia occurrence, surgical site occurrences (SSO), and SSI. Binomial tests were performed and Bonferroni penalties applied (p<0.01 was considered significant).
Results:
A total of 317 patients underwent LVHR repair. Within this cohort, patients had the following comorbidities: obesity (66.9%), recent tobacco use (8.8%), and diabetes (18.9%). Most patients had a ventral incisional hernia (61.2%) and 19.2% were recurrent. Hernias were on average 4.7±3.3 cm in width on preoperative imaging.
At a median follow-up of 21 (range 11-41) months, there was 1 (0.3%) lateral hernia and 13 (4.1%) hernia recurrences for an overall post-operative hernia occurrence of 14 (4.4%). Compared to expected rates in the literature, there were significantly fewer observed lateral hernias and hernia recurrences. There was no difference in the observed versus expected rates of SSI and SSO (Table).
Conclusion:
During LVHR, introduction of the mesh through a 10-12 mm port placed through the defect may decrease the prevalence of lateral hernias without increasing the risk of developing a SSI or recurrence. While further studies are needed to confirm these results, lateral 10-12 mm ports can be safely avoided during LVHR.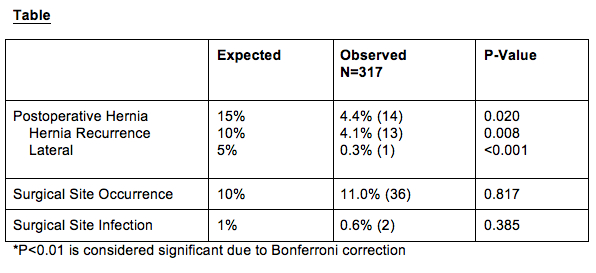
Back to 2019 Posters



