
DOES CONCOMITANT MECKEL'S DIVERTICULECTOMY ALONG WITH AN APPENDECTOMY INCREASE POSTOPERATIVE MORBIDITY?
Victor Vakayil*, Zachary D. Miller, Cassaundra K. Burt, James V. Harmon
Surgery, University Of Minnesota, Minneapolis, MN
Background
Meckel's diverticulitis can mimic acute appendicitis. There exists a considerable debate on the concomitant excision of a Meckel's diverticulum during an appendectomy. The risks of excision need to be weighed against the risk of developing postoperative complications and future diverticulitis. We evaluate the postoperative morbidity following the concomitant excision of a Meckel's diverticulum during an appendectomy.
Methods
We performed a 12-year retrospective review of the ACS-NSQIP database from 2005-2016 and identified patients undergoing Meckel's diverticulectomy and/or appendectomy using ICD-9/10 and CPT codes. Patients were then stratified into two cohorts; those undergoing an appendectomy with concomitant diverticulectomy (AM) and those undergoing an appendectomy alone (AA). To mitigate selection bias and adjust for baseline heterogeneity between groups, we used propensity-score matching with a case (AM): control (AA) ratio of 1:2. Both populations were matched on age, gender, demographics, severity of presentation including ASA scores, wound classification scores and various preoperative laboratory variables. We then compared intraoperative outcomes including operative time, 30-day postoperative outcomes including infectious and non-infectious morbidity, and 30-day postoperative mortality between groups.
Results
We identified 460 patients who underwent a concomitant Meckel's diverticulectomy during an appendectomy (AM). As compared to the AA group, on baseline, these patients had an increased proportion of baseline comorbidities with poorer preoperative labs. Propensity-score matching helped identify 460 matched controls from the AA group. Balance assessment demonstrated successful matching on all baseline characteristics. Postoperative outcome evaluation (Table 1) demonstrated the AM group to have increased operative time, with an increased duration of hospital stay (all P's <0.05). The rate of postoperative infectious morbidity including superficial, deep and organ space infections, urinary tract infections and rates of sepsis were similar between both groups (all P>0.05). Rates of non-infectious morbidity, reoperation, and mortality were also comparable between both groups (all P's >0.05).
Conclusions
In our review, concomitant Meckel's diverticulectomy with an appendectomy did not increase postoperative morbidity or mortality compared to appendectomy alone. However, clinical decision to excise a Meckel's diverticulum concomitantly during an appendectomy should be made on an individual basis based on the severity of presentation and comorbidity status.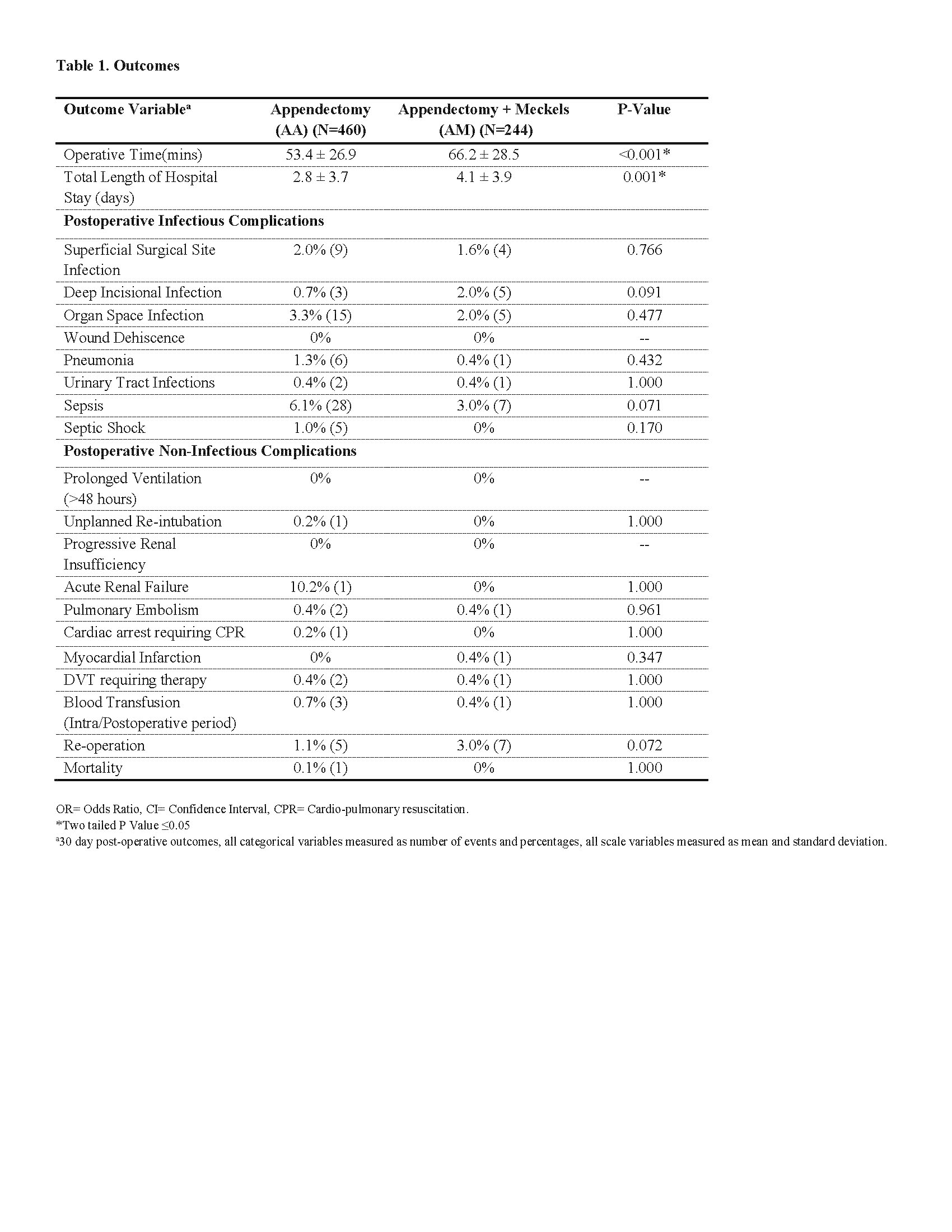
Back to 2019 Posters



