
ENDOSCOPIC MANAGEMENT OF ILEOCECAL VALVE LESIONS: IS IT FEASIBLE?
Ipek Sapci*, James M. Church, Emre Gorgun
Colorectal Surgery, Cleveland Clinic Foundation, Cleveland, OH
Background
Ileocecal valve lesions can be challenging to diagnose for two main reasons: they may not be easily separated from prolapsing small bowel mucosa, and lesions may extend behind the valve making excision technically difficult. We aimed to review the management of ileocecal valve lesions in a tertiary referral center and report our experience with endoscopic removal of these lesions.
Methods
All colonoscopies performed at a colorectal surgery department in a tertiary level hospital system between January 2010 and September 2018 were queried from a prospectively maintained institutional colonoscopy database. Colonoscopies during which an ileocecal valve lesion was reported were identified and demographics, examination findings, the technique of excision, immediate complications and pathology results were reviewed.
Results
42,259 consecutive elective colonoscopies were included in the study. Mean patient age was 63.1 ± 10.7 years and 54% of patients were female. 218 of scopes had ileocecal valve lesions that were biopsied or removed and that had a histopathological examination result. 24 lesions were biopsied only, and one underwent subsequent surgery due to a 30 mm tubulovillous adenoma. 194 lesions underwent removal with hot/cold biopsy forceps, snaring or advanced endoscopic resection. Median lesion size was 5 mm (IQR: 4, 15). Breakdown of management and final pathology of the lesions are given in the Table. The most common lesion was tubular adenoma, followed by tubulovillous adenoma. Six lesions were removed using advanced endoscopic techniques such as endoscopic mucosal resection and endoscopic submucosal dissection. There were no immediate complications reported. Four patients underwent surgery after endoscopic resection, 2 due to cancer and 2 due to advanced adenomas. Four patients had recurrences of the resected lesion and the recurrences were managed with subsequent endoscopic removal and there was no need for surgery.
Conclusion
Ileocecal valve polyps are rare but when found can be safely and effectively managed with biopsy forceps, snaring and advanced endoscopic techniques such for larger lesions as endoscopic mucosal resection or endoscopic submucosal dissection.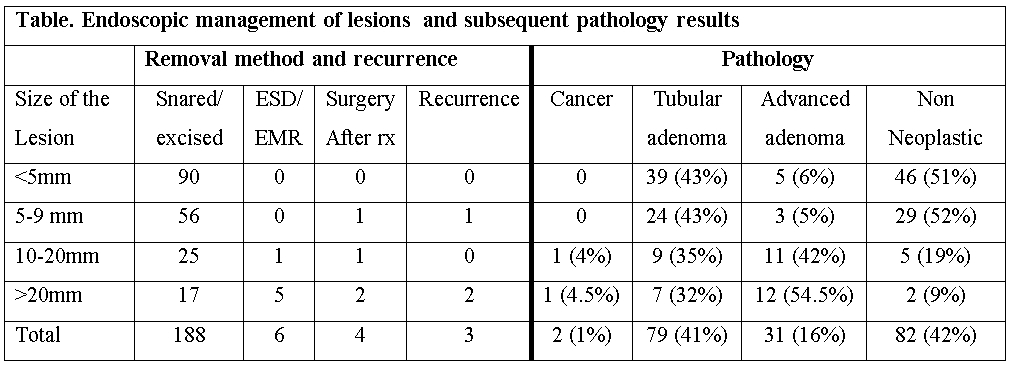
Back to 2019 Posters



