
SHORT AND LONG-TERM OUTCOMES OF PATIENTS WITH COLON CANCER OF THE SPLENIC FLEXURE: A SINGLE INSTITUTION EXPERIENCE
Esteban Calderon*1, Shreya Shetty2, Patrick T. Hangge1, Matthew Neville3, Scott Kelley4, Tonia Young-Fadok2, Etzioni David2, Nitin Mishra2
1Department of General Surgery, Mayo Clinic Arizona, Phoenix, AZ; 2Department of Colon and Rectal Surgery, Mayo Clinic Arizona, Phoenix, AZ; 3Department of Research and Biostatistics, Mayo Clinic Arizona, Phoenix, AZ; 4Department of Colon and Rectal Surgery, Mayo Clinic, Rochester, MN
Background: The optimal surgical resection for colon cancer of the splenic flexure is controversial. The purpose of this study was to compare short and long-term outcomes of segmental splenic flexure resection (SF) versus anatomical/oncologic resection (OR) in patients with splenic flexure adenocarcinoma.
Methods: A retrospective review of patients with newly diagnosed splenic flexure carcinoma from the year 1993 to 2015 was performed. Patients were stratified into segmental splenic flexure resection and anatomical/oncologic resection (extended right, left and subtotal colectomy) groups. Overall, 30 and 90 day mortality, overall survival, disease free survival, lymph node clearance and disease recurrence were compared.
Results: A total of 202 patients were found of which 113 underwent SF and 89 OR. There were no differences in age, gender, or race. For both groups, 77% of the operations were performed electively. The rest had urgent/emergent surgery for obstruction or perforation. Overall, 88% underwent primary anastomosis whereas 11% required either a colostomy or diverting loop ileostomy. Most operations were done open (81%). Most tumors overall were stage 2 and moderately differentiated although there was no difference between the two surgical groups. Lymphovascular invasion (LVI) and resection margins were comparable but OR had better mean lymph node clearance (17.6 vs 14.7, p=0.0047). No difference was identified in overall (p=0.12), 30 day (p=0.27) or 90 day mortality (p=0.32), overall survival (p=0.83), disease free survival (p=0.83) and overall recurrence (p=0.20). On Cox multivariable analysis, age (HR 1.07; 1.04-1.09, p=<0.001), and tumor stage (p=<0.001) were found to be significant factors affecting mortality, as expected.
Conclusion: Segmental splenic flexure resection outcomes are similar to anatomical/oncologic resection, making it a good option for the treatment of splenic flexure carcinoma. LVI, resection margins, mortality, survival, and recurrence are comparable when compared to formal oncologic resection. Lymph node clearance is statistically better but not clinically significant in a formal oncologic resection. The type of surgery offered to patients with this malignancy should be dependent on patient factors and surgeon preference.
Short and Long-Term Outcomes of Patients with Colon Cancer of the Splenic Flexure
| Variables | Anatomical/Oncologic Resection (N=89) | Segmental Splenic Flexure Resection (N=113) | Total (N=202) | p value | |
| Gender | Male | 55 (61.8%) | 63 (55.8%) | 118 (58.4%) | 0.3868 |
| Female | 34 (38.2%) | 50 (44.2%) | 84 (41.6%) | ||
| Age | 69 (27-88) | 71.4 (34-96) | 69.8 (27-96) | 0.0545 | |
| Reason for Surgery | Elective | 68 (76.4%) | 87 (77%) | 155 (76.7%) | 0.7533 |
| Obstruction | 16 (18%) | 19 (16.8%) | 35 (17.3%) | ||
| Perforation | 4 (4.5%) | 3 (2.7%) | 7 (3.5%) | ||
| Diversion | Anastomosis | 77 (86.5%) | 101 (89.4%) | 178 (88.1%) | 0.4537 |
| Colostomy | 9 (10.1%) | 11 (9.7%) | 20 (9.9%) | ||
| Ileostomy | 1 (1.1%) | 1 (0.9%) | 2 (1%) | ||
| Type of Surgery | Open | 67 (75.3%) | 97 (85.8%) | 164 (81.2%) | 0.1262 |
| Laparoscopic | 21 (23.6%) | 15 (13.3%) | 36 (17.8%) | ||
| Robotic | 1 (1.1%) | 0 (0%) | 1 (0.5%) | ||
| LN clearance | 17.6 (0-78) | 14.7 (0-98) | 16.0 (0-98) | 0.0047 | |
| Margins | Positive | 3 (3.4%) | 4 (3.5%) | 7 (3.5%) | 0.4920 |
| Negative | 86 (96.6%) | 106 (93.8%) | 192 (95%) | ||
| LVI | 11 (12.4%) | 6 (5.4%) | 17 (8.5%) | 0.0735 | |
| Mortality | Overall | 44 (49.4%) | 68 (60.2%) | 112 (55.4%) | 0.1274 0.2679 0.3184 |
| 30 day | 2 (2.2%) | 6 (5.3%) | 8 (4%) | ||
| 90 day | 4 (4.5%) | 9 (8%) | 13 (6.4%) | ||
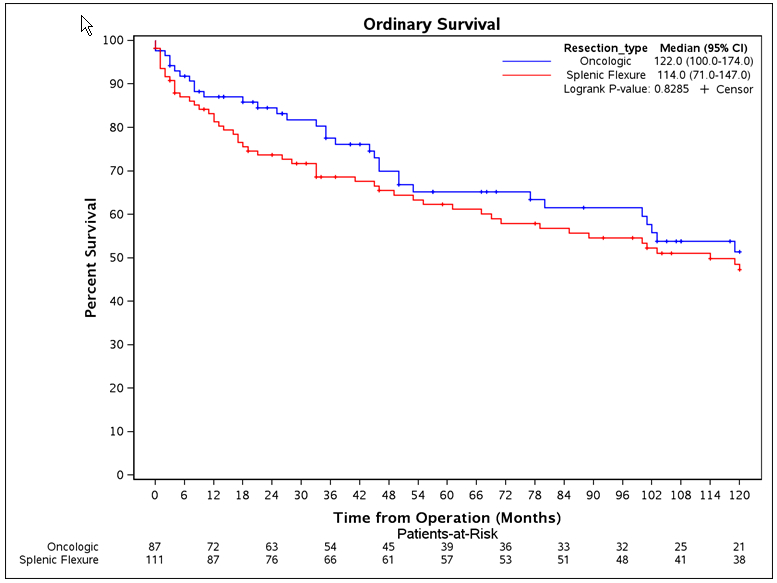
Splenic Flexure Versus Oncologic Resection - Overall Survival
Back to 2019 Posters



