
DOES HOSPITAL SETTING AFFECT THE DELIVERY OF BARIATRIC SURGICAL SERVICES WITHIN A HEALTHCARE SYSTEM
Cynthia Weber*, Rami R. Mustafa, LaCresha Warren, Mujjahid Abbas, Leena Khaitan
Surgery, University Hospitals of Cleveland, Cleveland, OH
Introduction Most healthcare centers offer bariatric surgical services (BSS) at a primary site. Within our system, we deliver BSS at three Centers of Excellence: urban academic center, suburban hospital and rural site. Patient preference determines location of surgery, except high-risk patients, who are referred to the urban center. We sought to characterize the populations at each hospital with regards to procedure performed and payer mix. We hypothesize that by utilizing a decentralized model, the system is better able to service the population and reach patients that otherwise would not have access to BSS.
Methods A retrospective review of an internally maintained database was performed for patients who underwent primary bariatric surgery (Vertical Sleeve Gastrectomy(VSG), Roux-en-Y Gastric Bypass(RYGB), Adjustable Gastric Band(AGB), Gastric Balloon) or revisional bariatric surgery from 2010-2018. Payer status was defined as private insurance, government insurance (Medicaid, Medicare and VA) or self-pay. Group A consists of patients who underwent BSS at the urban center; whereas Group B and Group C are patients who had surgery at the suburban hospital and rural site. Statistical analysis was performed using Chi-square; p<0.05 considered significant.
Results Private insurance was the predominant payer of the entire cohort, representing 63.4% (1716/2706 patients). No difference in gender exists between sites. Payer status differs by hospital (p<0.001); rural (Group C) and suburban (Group B) locations demonstrated higher private insurance coverage; 74.9% and 71%, respectively; compared to the urban center (Group A), where government insurance accounts for 46.1%. Only 28.2% in Group B and 21.5% in Group C had government insurance. Medicaid was more common than Medicare. Zip codes were similar at A and B, but very different in Group C. The rural site saw the largest percentage of self-pay patients. We detected a significant difference in type of bariatric procedure (p<0.001). While VSG was the most common bariatric operation in Groups A and B; RYGB was the primary operation in Group C. The rate of revisional surgery was highest at the academic center (Group A), accounting for 10.5% of all procedures; compared to 4.5% and 4.9% in Groups B and C, respectively.
Conclusion This study demonstrates that distributing BSS across hospital environments allows for a broad delivery of BSS. Patients tend to choose the hospital that is closest to them. While private insurance covers the largest percentage of patients, as expected, our urban academic center sees a higher proportion of patients with government insurance and more revisional bariatric surgery. Patients in the rural hospital undergo RYGB most commonly. While the reasons for these differences are not clear, we hypothesize that decentralization across a system can allow BSS to be delivered to more patients.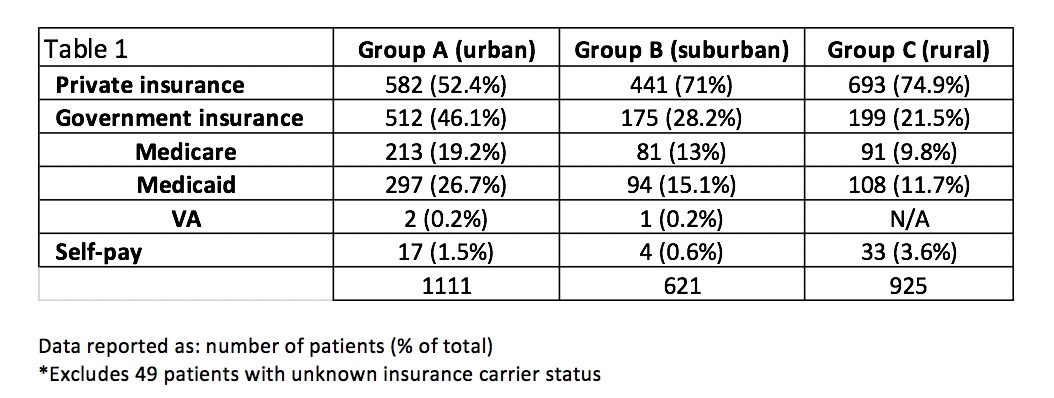

Back to 2019 Posters



