
DOES SURGICAL INTERVENTION REDUCE MORTALITY IN CLOSTRIDIUM DIFFICILE RELATED TOXIC MEGACOLON?
Abhinav Goyal*1, Kshitij Chatterjee2, Surbhi Abrol3, Janani Rangaswami4, Shailender Singh5
1Department of Digestive Diseases and Transplantation, Einstein Medical Center, Philadelphia, PA; 2Respiratory Institute, Cleveland Clinic, Cleveland, OH; 3Smile Kraft, Dharamshala, India; 4Internal Medicine, Einstein Medical Center, Philadelphia, PA; 5Division of Gastroenterology, Deptt. of Internal Medicine, University of Nebraska Medical Center, Omaha, NE
INTRODUCTION
Toxic megacolon, a rare but dreaded complication of Clostridium difficile colitis (CDI), is defined as colonic distension of >6cm with acute colitis and signs of systemic toxicity. Toxic megacolon is a rare complication of CDI because of which there are no large scale studies available. Our aim is to identify the effect of surgical intervention on mortality in patients with toxic megacolon secondary to CDI, in a national population.
METHODS
National Inpatient Sample for years 2009-2013 was used for this study. It is the largest ICD-9 code based inpatient database in the US. ICD-9-CM code 008.45 was used to identify all adults with CDI. Toxic megacolon was identified with ICD-9-CM code 558.2. Similarly, surgical interventions were identified using ICD-9-CM procedure codes. All hospitalizations with missing age or gender information were excluded. Demographic characteristics and outcomes were summarized using mean/median for continuous variables and percentages for categorical variables. Multivariate cox proportional hazards regression was used to identify the predictors of mortality. Age, gender, hospital characteristics, clinically relevant co-morbidites, surgical intervention, time to surgery were considered for univariate analysis. All covariates with p<0.10 on univariate analysis were included in multivariate analysis. Data was right censored at discharge. Stata 14.0 (Stata corp., Collegetown, TX) and SPSS 23.0 (SPSS Inc., Chicago, IL) were used for all statistical analysis.
RESULTS
A total of 1,672,600 cases of CDI were identified between 2009 to 2013. 926 (0.06%) of these had toxic megacolon. 482 (52.1%) of these received surgical intervention and 279 (30.2%) died during their hospitalization. Mean time to surgery was 4.8 ± 0.6 days. 126 (13.6%) patients died despite surgical intervention. Mean age was 67.8 years, 55.7% were females, and median length of stay was 13 days. On multivariate cox regression, surgical intervention was associated with a lower hazard of mortality (HR=0.5, p=0.04) and diabetes was associated with a greater hazard of mortality (HR=2.1, p=0.04). Mean time to surgery was 4.8 ± 0.6 days.
CONCLUSION
Toxic megacolon is a very rare complication of CDI but is associated with a significant mortality of 30.2%. This is the first study to describe the mortality and its risk factors in a national population.
Diabetes (HR=2.1) was one of the risk factors for in-hospital mortality and surgical intervention (HR=0.5) significantly lowered the risk of mortality.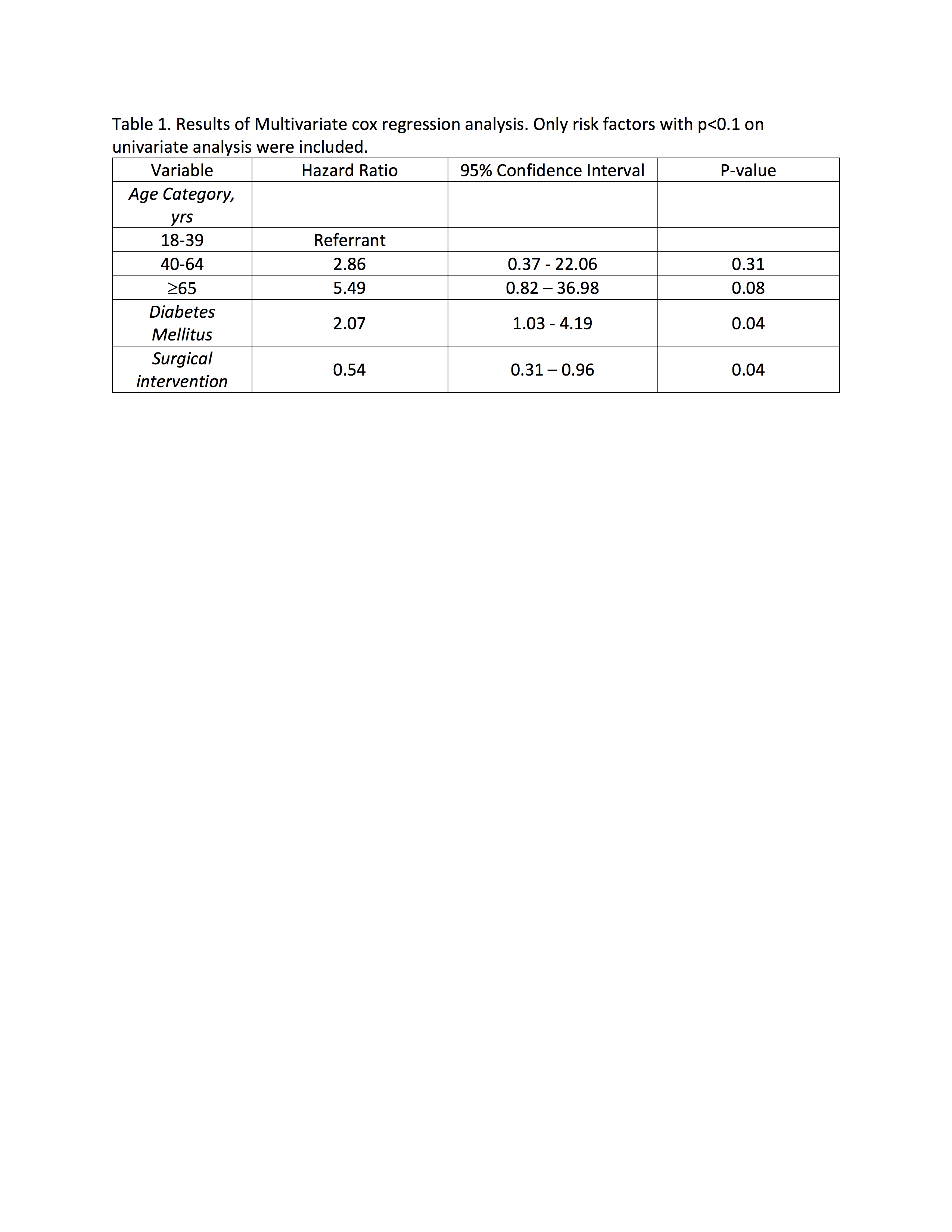
Back to 2019 Abstracts



