
OUTCOMES AFTER IMPLEMENTATION OF A SURGICAL CARE BUNDLE FOR COLECTOMY FOLLOWED BY ENHANCED RECOVERY PROTOCOL FOR PATIENTS WITH INFLAMMATORY BOWEL DISEASE UNDERGOING COLORECTAL RESECTION
Anthony D'Andrea*, Prerna Khetan, Reba Miller, Patricia Sylla, Celia M. Divino
General Surgery, Mount Sinai Hospital, New York, NY
Objective:
To compare outcomes before and after implementation of a hospital-wide surgical care bundle (SCB) for colectomy followed by enhanced recovery protocol (ERP) for patients with inflammatory bowel disease (IBD) undergoing colorectal resection.
Background:
Preoperative SCBs for colectomy are comprised of a small set of evidence-based practices proven to reduce rates of surgical site infection (SSI). They were supplemented with ERPs, which are perioperative care pathways designed to minimize the physiologic stress of surgery and accelerate postoperative recovery. Together, SCBs and ERPs lower rates of surgical site infection (SSI), ileus, and length of hospital stay for patients undergoing colectomy or proctectomy. However, their impact on patients with IBD is understudied.
Methods:
All patients with Crohn's disease or ulcerative colitis undergoing elective colectomy or proctectomy at a tertiary-level referral center from 2013-2018 were retrospectively evaluated using ACS-NSQIP data. Postoperative outcomes at 30 days were compared between pre-SCB/ERP, post-SCB, and post-SCB+ERP cohorts. Pediatric (age <18 years) and emergency cases were excluded. Components of the SCB and ERP programs are listed in Table 1.
Results:
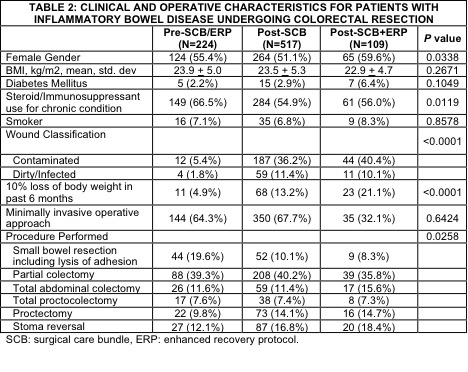
Out of 850 patients, 224 were pre-SCB/ERP, 517 were post-SCB, and 109 were post-SCB+ERP. On univariate analysis, gender (P=0.038), immunosuppressant use (P=0.0119), wound classification (P<0.001), malnutrition (P<0.001), and procedure performed (P=0.0258) were significantly different between the three cohorts (Table 2). After adjusting for these variables using multivariable logistic regression, SSI showed a persistent, statistically significant decline post-SCB (OR 1.77, CI 1.032-3.038) and post-SCB+ERP (OR 2.527, CI 1.032-6.188). Ileus decreased significantly only post-SCB (OR 2.575, CI 1.551-4.273).
Conclusion:
Implementation of SCB for colectomy demonstrated improvement in rates of SSI and ileus for IBD patients undergoing elective bowel resection. The benefit for SSI rates increased in the era of enhanced recovery.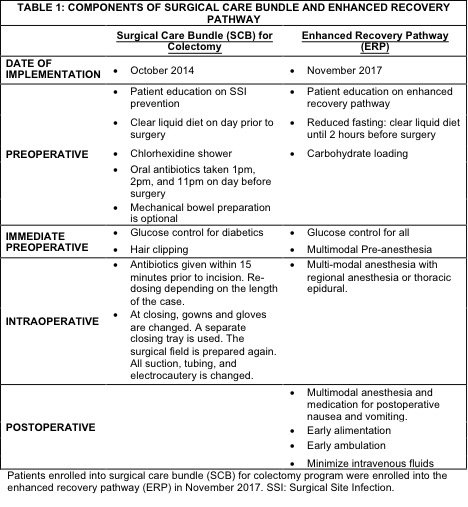
Back to 2019 Abstracts



