
ENDOSCOPIC CLOSURE VERSUS SURGICAL REVISION IN THE MANAGEMENT OF GASTROGASTRIC FISTULA FOLLOWING ROUX-EN-Y GASTRIC BYPASS
Ethan D. Maahs*, Pichamol Jirapinyo, Christopher C. Thompson
Brigham & Women's Hospital, Boston, MA
Background: Gastrogastric fistula (GGF) is a rare but important complication of Roux-en-Y gastric bypass (RYGB). Symptoms may include abdominal pain, acid-related diseases and weight regain. Surgical revision has traditionally been employed to revise and treat GGF. Alternatively, endoscopic closure of GGF may be performed as a less invasive approach.
Aim: To compare outcomes of endoscopic closure and surgical revision of GGF in RYGB patients.
Methods: This was a retrospective matched cohort study of RYGB patients who underwent endoscopic closure (ENDO) or surgical revision (SURG) for GGF at two tertiary referral centers. ENDO patients were matched 1:1 to SURG patients based on age, sex, body mass index (BMI) and weight regain. Patient demographics, GGF size, procedural details, symptoms related to GGF and serious adverse events (SAEs) were collected. Collected symptoms included abdominal pain, acid reflux and weight profile. Weight regain was defined as gaining of at least 15% of the maximal weight loss. Outcomes: Proportions of patients with symptom improvement after ENDO or SURG were compared. Additionally, SAE rate of the two groups were analyzed. Statistics: A chi squared and Student's t-test were used.
Results: 90 RYGB patients with GGF (45 ENDO, 45 matched SURG) were included (Table 1). Average GGF size was 15±9 mm and average time from RYGB was 8.9±5.3 years. Symptoms of GGF included weight regain (80%), GERD (71%) and abdominal pain (67%). Weight regain: At 6 months, 78% of the ENDO group and 89% of the SURG group stopped gaining weight (p=0.23). At 6 months, the ENDO and SURG groups experienced 1.04% and 2.56% total weight loss (TWL) (p=0.18), respectively. At 12 months, 59% of the ENDO group and 93% of the SURG group stopped gaining weight (p=0.007). At 12 months, the ENDO and SURG groups experienced 0.60% and 4.63% TWL (p=0.0003), respectively. GERD: GERD symptoms improved in 16% for ENDO versus 6% for SURG (p=0.20). Abdominal pain: Abdominal pain improved in 57% for ENDO versus 16% for SURG (p=0.001). Serious adverse events: The SAE rates for ENDO and SURG were 8.9% and 35.6% (p=0.005), respectively. SAEs in the ENDO group included marginal ulceration (3) and severe abdominal pain (1). SAEs in the SURG group included leak (4), abdominal hernia (3), abscess (3), severe abdominal pain (3), GI bleeding (1), small bowel obstruction (1) and gastrojejunal anastomotic stricture (1).
Conclusion: Endoscopic closure of GGF results in greater improvement in abdominal pain with similar efficacy for GERD symptoms and fewer serious adverse events. However, surgical revision appears to yield greater weight loss.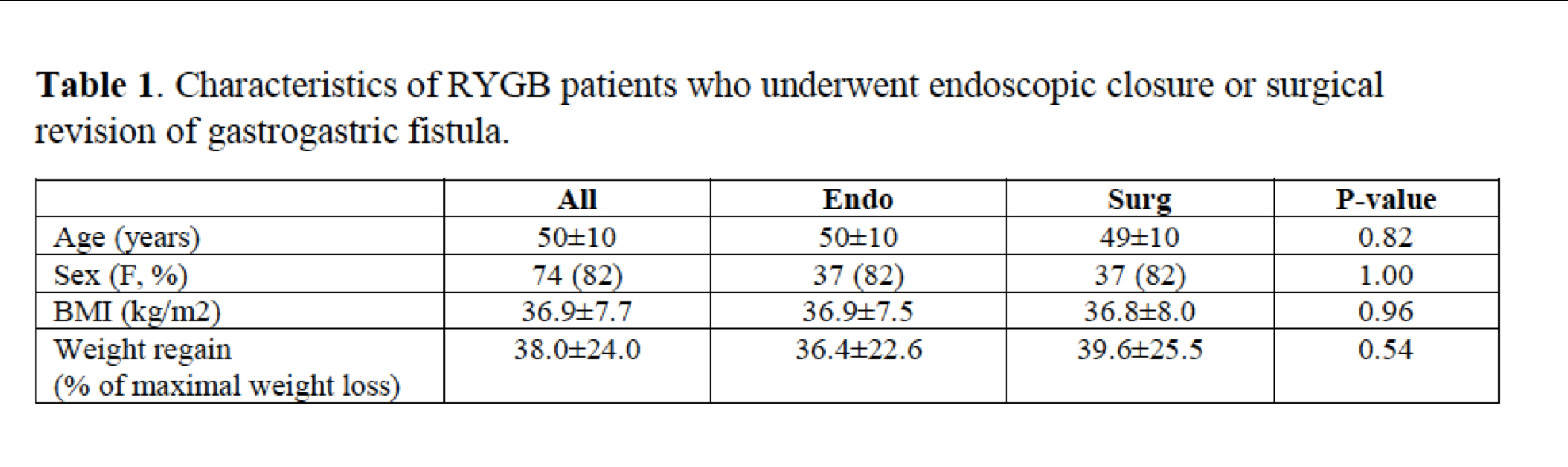
Back to 2019 Abstracts



