
JEJUNOSTOMY FEEDING TUBES FOLLOWING COMPLEX FOREGUT/HPB SURGERY: ARE THEY REALLY SUCH A HASSLE?
Conor H. O'Neill*, Robert C. Martin
University of Louisville, Louisville, KY
Introduction: Perioperative nutrition remains integral for successful outcomes and the return to baseline quality of life. Following complex foregut surgery, jejunostomy feeding tubes (J-tube) may be required to ensure enteral feeding access and adequate nutritional support. Our bias is liberal use of postoperative feeding tube access, especially in the setting of foregut reconstruction and adjuvant therapy. We review our experience with J-tube placement following foregut surgery.
Methods: We performed a review of our J-tube placements from 1/1/2010 until 7/1/2018. Indication for surgery, primary operation and comorbidities, including diabetes, cardiopulmonary disease, hypertension and presence of vasculopathy were recorded. Adverse events related to the J-tube were noted. Social "hassle-factor"? issues are reported, including number of "˜J-tube-related' phone calls, reinsertion and related placement studies, and readmissions pertaining to J-tube associated complications. Lastly, the number of days from initial placement until removal was noted.
Results: 546 J-tube placements were performed during 21 subtotal pancreatectomies, 38 distal pancreas resections, 110 Whipple procedures, 100 ablations, 14 distal gastrectomies, 145 esophagogastrectomies, 5 diagnostic laparoscopies, 7 partial gastrectomies, 39 total gastrectomies, 19 splenectomies, 36 diaphragm resections and 12 liver resections. There were 180 J-tube related adverse events. Dislodged tubes occurred in 36% (n=65), followed by clogged tubes 16% (n=30), leaking tubes 14% (n=25), 15 site infections, 9 pain events, 7 related to intolerance, 10 malfunctions/drainage issues, 9 tube breaks, 8 loose tubes at exit site, 1 event related to malnutrition despite tube, and 1 event related to bleeding. There were 272 reinsertion/placement studies and 27 J-tube related readmissions. There was a significant difference in adverse events between groups (p<0.0005): esophageal and gastric resections had an adverse event rate of 40%, while subtotal pancreatectomies and liver resections had an event rate of approximately 10%. There was no difference in the frequency of J-tube related phone calls to providers with respect to procedure type (p=0.33). Length of time with J-tube was roughly equivalent between all groups. All adverse events resolved prior to removal of the tube.
Discussion: J-tubes have complications. We report a cumulative 180 adverse events and 272 insertion/placement studies during the life of the tube in 546 procedures necessitating placement. Despite these challenges, the number of days requiring J-tube was roughly equivalent between populations. Collectively, while these tubes do cause a high rate of adverse events, these events do not seem to influence clinical practice. This finding highlights the imperative for adequate postoperative nutrition and enteral access.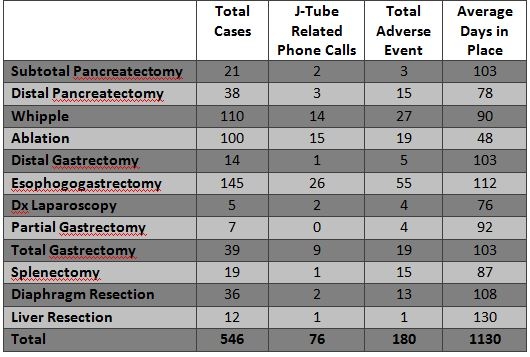
J-tube related complications
Back to 2019 Abstracts



