
ROLE OF SURGICAL RESECTION IN THE ERA OF FOLFIRINOX FOR ADVANCED PANCREATIC CANCER
Yoonhyeong Byun*, Youngmin Han, Mirang Lee, Hongbeom Kim, Wooil Kwon, Sun-Whe Kim, Jin-Young Jang
Surgery, Seoul National University Hospital, Seoul, Korea (the Republic of)
The introduction of FOLFIRINOX treatment in patients with advanced pancreatic cancer that led to a major change in the therapeutic paradigm. Recently, the number of attempts for active surgical resection after downstaging of advanced lesions is increasing; however, the effects of FOLFIRINOX, the role and timing of surgery after the FOLFIRINOX treatment, and the analysis on prognostic factors is limited. The purpose of this study is to evaluate the effects of FOLFIRINOX and the role of surgical treatment in the era of FOLFIRINOX against advanced pancreatic cancer.
Patients pathologically diagnosed with advanced pancreatic cancer who received the FOLFIRINOX chemotherapy at Seoul National University Hospital (SNUH) from January 2011 to December 2017 were reviewed retrospectively. Among them, 342 patients were finally appropriate for this study. All radiologic images were re-reviewed, the clinical stages was reclassified by NCCN guideline. After 4-6 cycles of treatment, each cases were classified according to the RECIST criteria 1.1 for the assessment of a response, and further treatment was decided in the multidisciplinary meeting.
A total of 68 (19.9%) patients had borderline resectable pancreatic cancer (BRPC), 126 (36.8%) locally advanced pancreatic cancer (LAPC), and 148 (43.3%) metastatic pancreatic cancer. Regarding the response after FOLFIRINOX, 107 (31.3%) had partial response (PR), 187 (54.7%) stable disease (SD), and 48 (14.0%) progressive disease (PD). Those who achieved SD was 45 (66.2%) in BRPC, 69 (54.8%) in LAPC, and 73 (49.3%) in metastatic stage. The median survival period was significantly longer in the surgical group than in the nonsurgical group in each clinical stage: BRPC, 33 vs. 14 (p=.011); LAPC, 27 vs. 15 (p=.002), and metastatic pancreatic cancer, 34 vs. 13 months (p=.010). In multivariate analysis, metastatic stage (p=.020), PD after FOLFIRINOX (p<.001), and curative operation (p<.001) were significant prognostic factors.
This study clearly showed that the surgical treatment greatly affects survival outcomes in advanced pancreatic cancer treated with FOLFIRINOX, even for the metastatic ones. Therefore, if the disease progression is controlled after FOLFIRINOX treatment in patients with advanced pancreatic cancer, including metastatic stage, surgical resection should be actively attempted to improve the survival outcome. As the tumor markers in our multivariate analysis were marginally significant, it could be considered to evaluate the resectability. In order to attempt curative resection, a factor that exerts great influence on the survival outcome, other treatment modalities that were proven to be more effective, such as radiotherapy, should be introduced. Future clinical studies are required to identify the optimal neoadjuvant regimens and indications of surgical resection in advanced pancreatic cancer.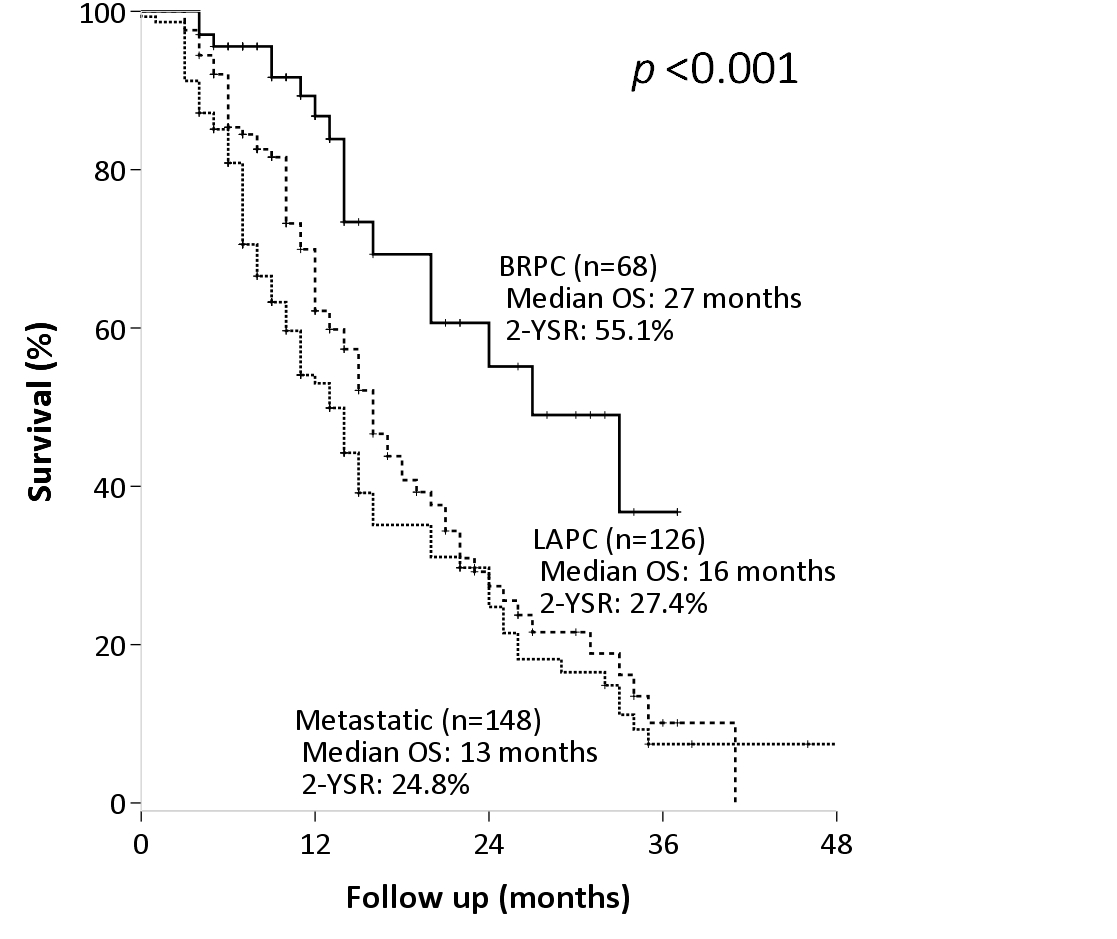
Survival analysis by the clinical stage at the clinical diagnosis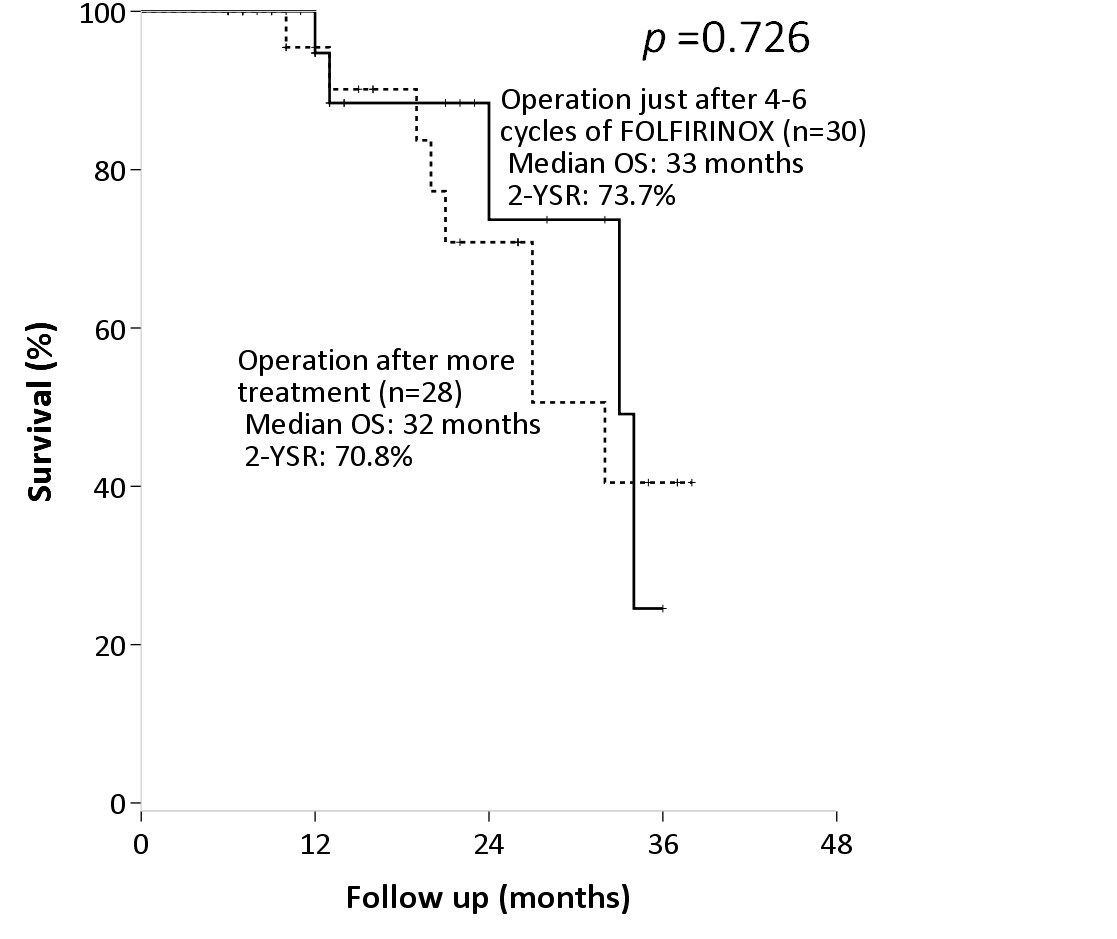
Survival analysis according to the time of the operation.
Back to 2019 Abstracts



