
INDEX-CHOLECYSTECTOMY FOR MODERATE TO SEVERE BILIARY ACUTE PANCREATITIS DECREASES RECURRENCE OF GALLSTONES-RELATED DISEASES.
C. Roberto Simons-Linares*1, Miguel Salazar2, James S. Ramey1, Isaac Paintsil2, Prabhleen Chahal1
1Gastroenterology and Hepatology, Cleveland Clinic, Cleveland, OH; 2Internal Medicine, John H. Stroger Hospital of Cook County, Chicago, IL
Background & Aim: Same admission cholecystectomy (CCY) for mild biliary acute pancreatitis (BAP) is recommended. However, timing for CCY in moderate to severe BAP is controversial and literature is very limited. Moreover, the existing studies did not utilize updated definition for severity of AP. We sought to investigate the safety and outcomes of moderate to severe BAP patients undergoing same admission and post discharge CCY.
Methods: Retrospective cohort at a tertiary center between 2012 to 2017 of patients with moderate to severe BAP, according to the Revised Atlanta Classification. We stratified two groups: index-cholecystectomy (IC, same admission) and interval-delayed-cholecystectomy (IDC, after at least 1 week post-discharge). Multivariable logistic regression models using SAS software version 9.4
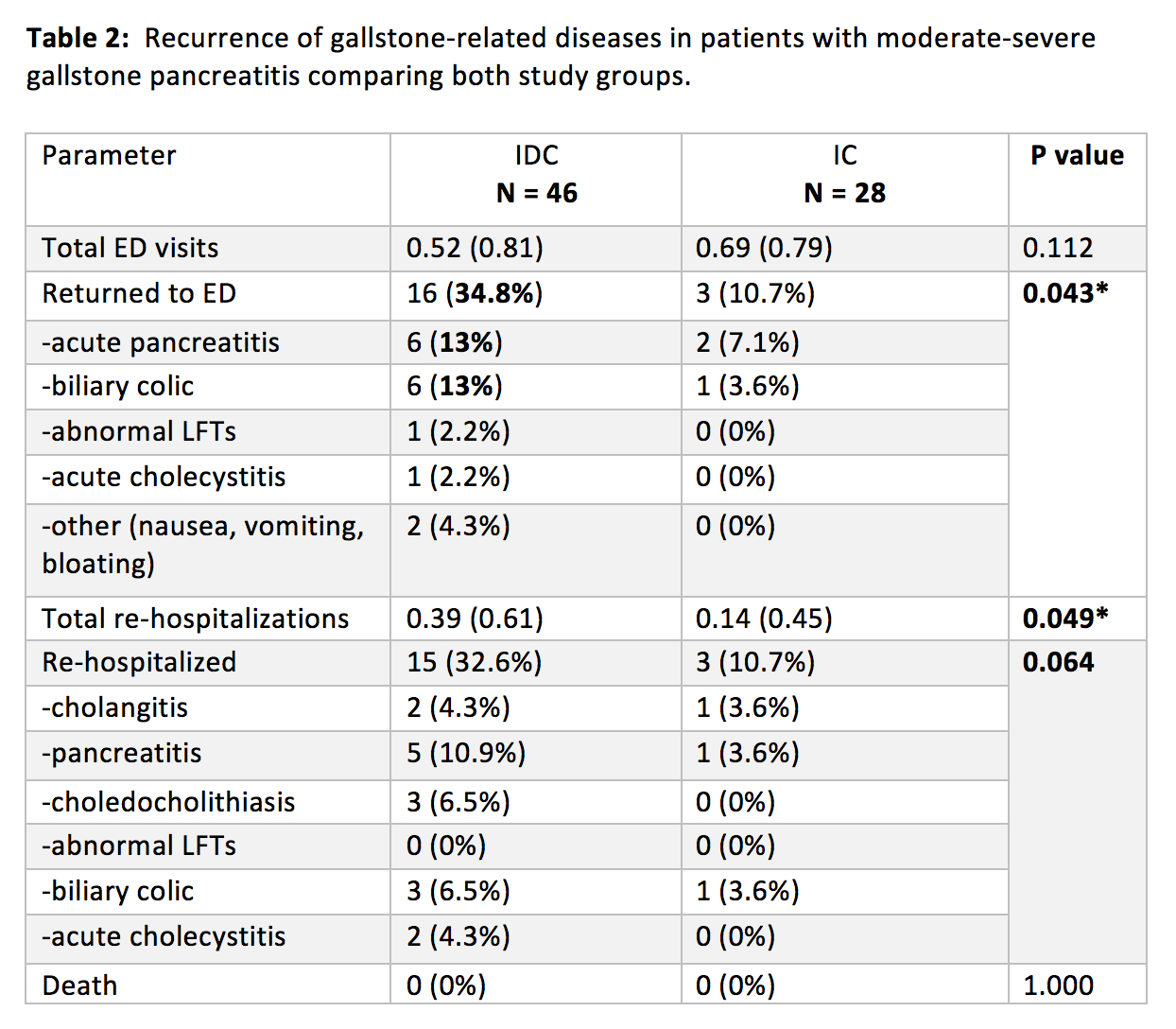
Results: A total of 531 patients were evaluated, of whom 74 were diagnosed with moderate to severe BAP. 28 (38%) underwent IC and 46 (62%) underwent IDC. IDC were more likely to be males (54% vs. 25%, p=0.026), but there were no other significant differences in baseline characteristics between the two groups (table 1a). The median time for IDC was 27.5 days (7-371). IDC patients significantly higher rates of emergency department (ED) visits related to gallstone diseases (34.8% vs. 10.7%, p=0.043), re-hospitalizations (32.6% vs 19%, p=0.064), recurrent pancreatitis (13% vs. 7.1%), biliary colic (17.4% vs. 3.6%), choledocholithiasis (6.5% vs. 0%). Two patients (4.3%) we re-hospitalized due to acute cholecystitis in the IDC group. Re-hospitalization for cholangitis rates were similar (4.3% vs. 3.6%) between the two groups. There were no post operative complications.
Conclusion: Same admission CCY should be performed in patients with moderate to severe biliary acute pancreatitis in order to avoid further undesired gallstone-related ED visits and re-hospitalizations for recurrent acute pancreatitis, biliary colic, choledocholithiasis and acute cholecystitis. Importantly, this cohort study demonstrates that CCY can be safely carried out even in patient with moderately severe AP complicated by pancreatic fluid collection formation.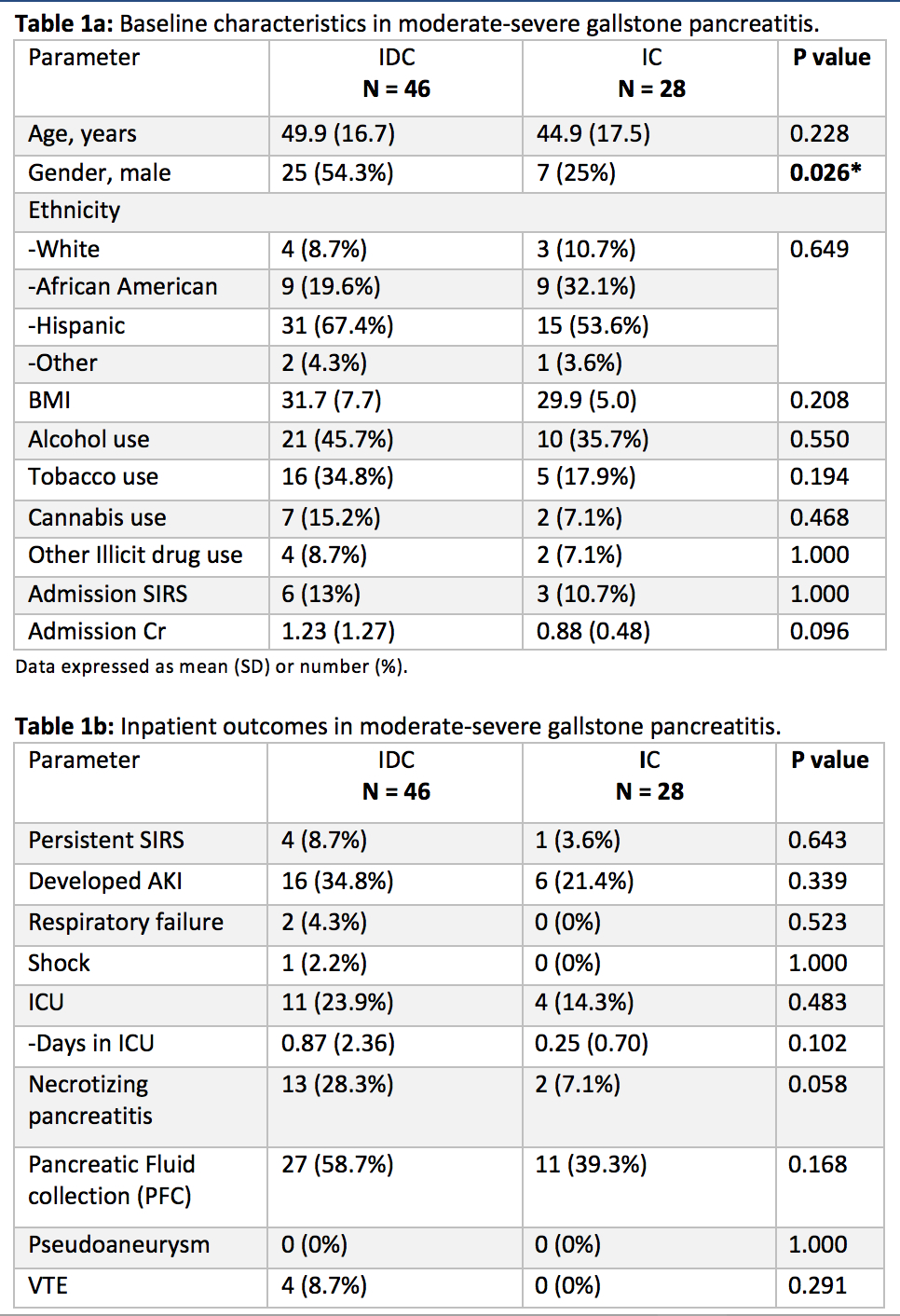
Back to 2019 Abstracts



