|
Back to 2014 Annual Meeting Posters
Endoscopy in the Immediate Postoperative Setting After Primary Gastrointestinal Anastomosis
Mahmoud Amr*, Mohammad J. Alzghari, Mohammad a. Khasawneh, Todd H. Baron, David S. Morris, Donald Jenkins, Martin D. Zielinski
Trauma, Critical Care and General Surgery, Mayo Clinic, Rochester, MN
Introduction: Gastrointestinal anastomoses in the early postoperative period may require evaluation and treatment via flexible endoscopic techniques when complications arise. There is reticence, however, to perform endoscopy given the mechanical forces from torque and air insufflation. We aimed to identify the incidence of gastrointestinal anastomotic perforation resulting from endoscopy performed ≤6 weeks of anastomoses.
Methods: Review of patients from 2002 to 2013 who underwent flexible endoscopy within six weeks of a gastrointestinal anastomosis. Exclusion criteria included intraoperative endoscopy, anastomotic perforation prior to endoscopy, and endoscopy remote from the anastomotic site. Data are presented as median (interquartile range; IQR) or percentages as appropriate.
Results: There were 11578 patients with gastrointestinal anastomoses performed during the study period of whom 24 (0.2%) underwent endoscopy in the postoperative period (age 69 years [IQR 54-77], 54% men]). Of these patients, there were 33 anastomoses performed (12 small intestine, 8 colocolic, 5 ileocolic, 1 jejunocolic, 3 esophagogastric, 2 gastrojejunal, 1 gastrocolic, 1 bilioduodenal). Indications for the index operation included cancer treatment, small bowel obstruction, inflammatory bowel disease, mesenteric ischemia and bowel perforation. Median endoscopy was performed on postoperative day 19 (IQR 8-34) with 15 patients (63%) undergoing colonoscopy and 9 (37%) upper endoscopy, (71%) of the endoscopies traversed the anastomosis site. Indications for endoscopy included bleeding (67%), obstruction (13%), pain (8%), cancer surveillance (4%), and concern for ischemia (4%). Four patients underwent therapeutic endoscopic procedures including coagulation (8%), balloon dilation (8%), and stent placement (4%). Mortality was 13%, none of whom were due to endoscopy. There were no anastomotic perforations as a result of endoscopy.
Conclusion: Postoperative flexible endoscopy for management of anastomotic complications is performed infrequently. Despite the theoretical risk of adverse events of endoscopy, no endoscopic perforations occurred in recently created surgical anastomoses, which denotes the safety of the procedure.
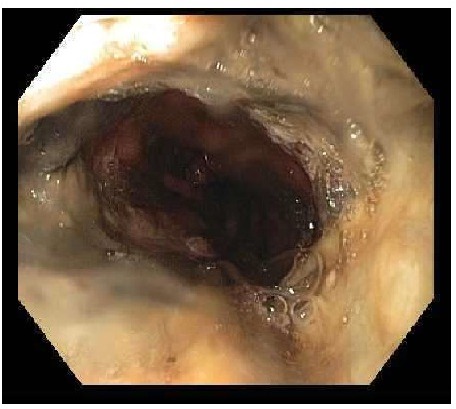
 EGD post Ivor-Lewis
Back to 2014 Annual Meeting Posters
|