|
Back to 2014 Annual Meeting Posters
Anti-Reflux Surgery Before Lung Transplantation Is Associated With Decreased Early Rejection Compared to Surgery After Transplantation
Wai-Kit Lo*1,2, Robert Burakoff1, Natan Feldman1, Walter W. Chan1
1Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women's Hospital, Boston, MA; 2Gastroenterology Section, Boston VA Healthcare System, Boston, MA
Background: Anti-reflux surgery (ARS) has been associated with improved long term outcomes following lung transplantation. Pre-transplant ARS has been shown in small studies to improve pulmonary function among transplant candidates with evidence of reflux. The optimal timing of ARS in transplant recipients, whether before or after transplantation, has not been assessed previously.
Aim: To evaluate the time to early acute rejection between lung transplantation patients undergoing ARS before versus after transplantation.
Methods: This was a retrospective cohort study of lung transplant recipients undergoing ARS before or after transplantation at a tertiary care center since 2007, with follow-up time of at least one year. Early acute rejection was defined clinically and histologically as allograft rejection occurring within the first year after transplantation. Both cumulative incidence and time-to-event analysis using the Cox proportional hazards model were applied to assess the relationship between timing of surgery and rejection. Subjects not meeting this outcome were censored at one year in the time-to-event analysis. Fisher's exact test for binary variables and student's t-test for continuous variables were performed to assess for differences between surgical timing groups.
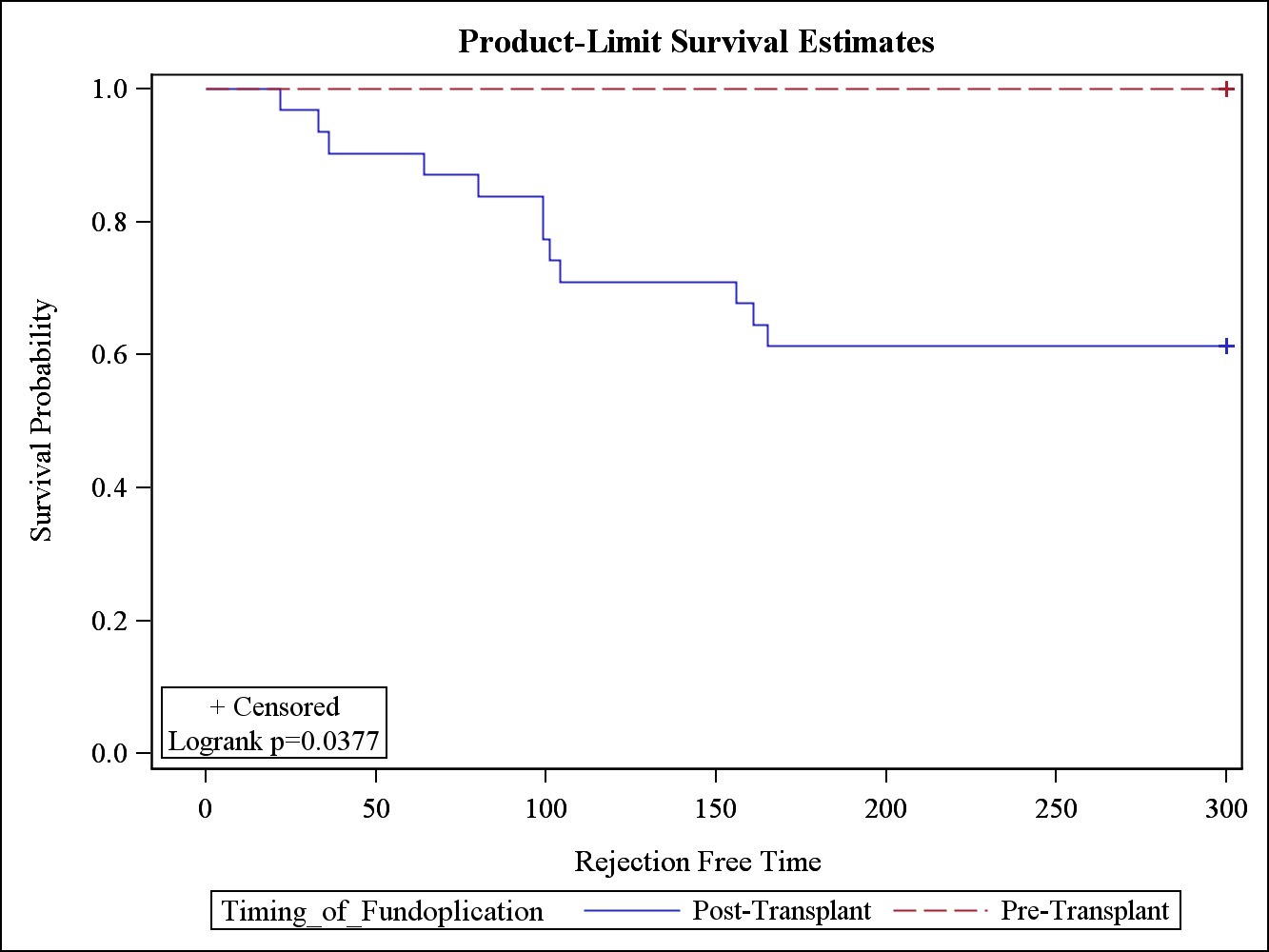
Results: 40 subjects (62% men, mean age: 54, average follow-up: 3.1 years) met inclusion criteria for the study. Patient demographics, pre-transplant cardiopulmonary function, BMI, CMV status, and PPI exposure were similar between pre- and post- transplant ARS groups. Pre-transplant ARS was associated with a significantly lower rate of early acute rejection within the first year post-transplant compared to post-transplant ARS (0% versus 39%, p=0.03). Time-to-event analysis showed similar decrease in risk of acute rejection by pre-transplant ARS compared to post-transplant ARS (log-rank p=0.04). ARS was overall tolerated well in both groups, with no complications noted in the pre-transplant group. One subject in the post-transplant group died two weeks post-ARS from aspiration pneumonia. A second required surgical conversion after one month due to regurgitation symptoms.
Conclusion: Pre-lung transplant ARS decreased the risk of early acute rejection following lung transplantation compared to post-transplant ARS. Exposure to reflux, even in the early post-transplant period, may have significant impact on allograft injury, inflammation, and survival. ARS was overall safe among our cohort of lung transplant patients. Additional prospective studies should be performed to further identify the optimal candidates and timing for ARS in the lung transplant population. Pre-lung transplant ARS may be considered in suitable lung transplant candidates with objective signs of reflux on pre-transplant assessment.
 Figure 1. Kaplan-Meier Analysis of time to early rejection by timing of fundoplication. Post-transplant surgical fundoplication was associated with early rejection.
Back to 2014 Annual Meeting Posters
|