|
Back to 2014 Annual Meeting Posters
Development of a New Preoperative Staging System for Prediction of Resectability in Hilar Cholangiocarcinoma
Jim Wiggers*1, Anthony T. Ruys1, Robert-Jan S. Coelen1, Erik Rauws2, Olivier R. Busch1, Dirk Gouma1, Thomas M. Van Gulik1
1Surgery, Academic Medical Centre, University of Amsterdam, Amsterdam, Netherlands; 2Gastroenterology, Academic Medical Centre, University of Amsterdam, Amsterdam, Netherlands
Background: Radical surgical resection offers the best long-term survival in hilar cholangiocarcinoma (HCCA). We aimed to assess the value of a staging system based on previously described prognostic factors available from preoperative imaging to predict the chance of obtaining a radical (R0) resection.
Methods: A total of 180 patients underwent explorative laparotomy for HCCA at a single, tertiary care center. If no distant metastases were found and the tumor appeared to be locally resectable, resection with curative intent was performed using extrahepatic bile duct resection with partial liver resection. The cohort was divided in a training set (n=116) treated between 2003-2009 and a validation set (n=64) treated between 2010-2013. A staging system to predict R0 resection based on preoperative imaging parameters (bilateral second order biliary involvement, vascular or lymph node involvement) was derived from previously described prognostic factors in the training set. The area under the receiver operating characteristic curve (AUC) was used to assess the discrimination achieved by the staging system.
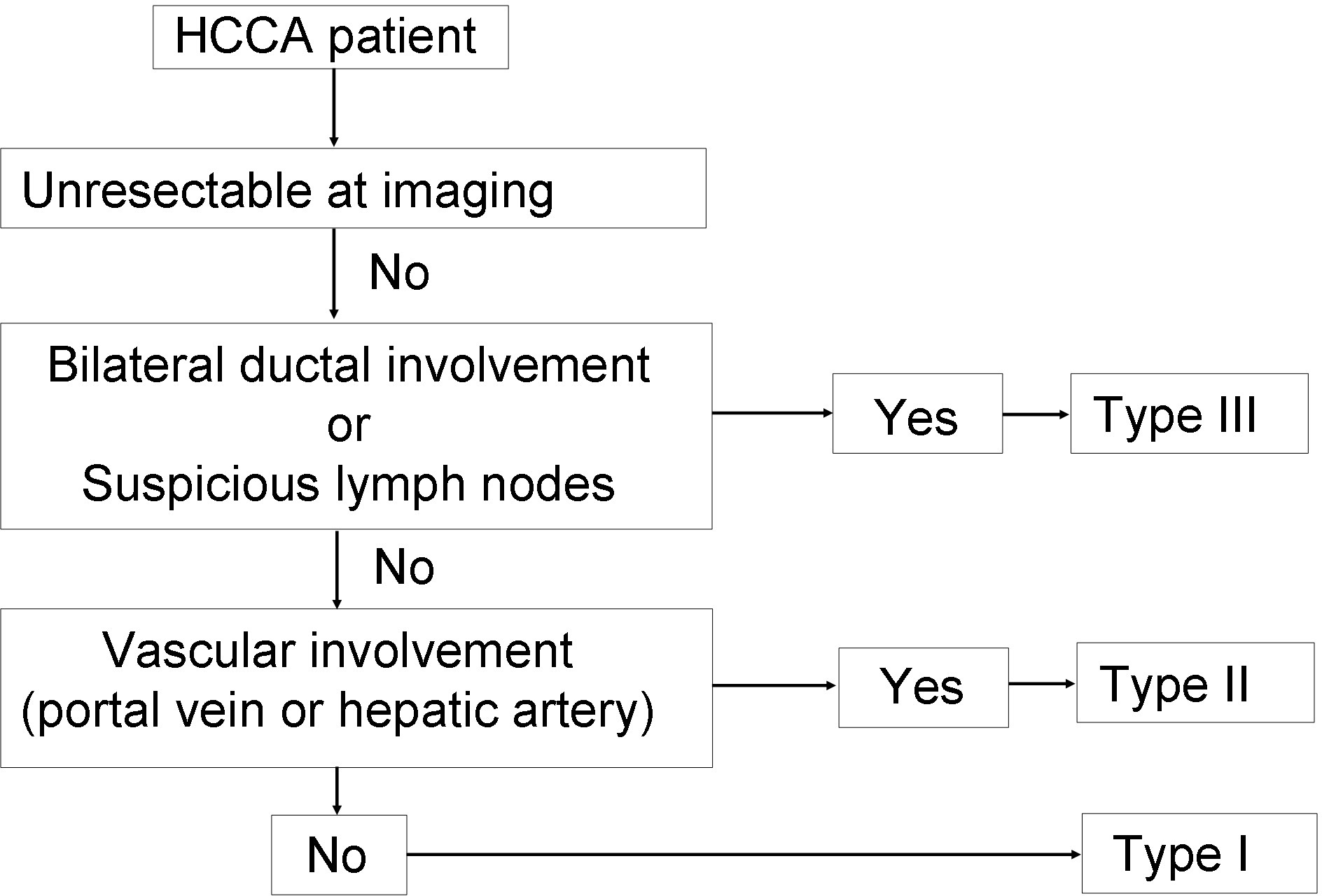
Results: Of 180 patients, a resection was performed in 104 patients (58%), which was a R0 resection in 88 patients (49%). Patients were stratified according to the proposed preoperative staging system (Figure 1). R0 resection rate was 72% in preoperative HCCA Stage 1 (33 of 46 patients), 44% in preoperative HCCA Stage 2 (27 of 61 patients), and 38% in preoperative HCCA stage 3 (28 of 73 patients). The AUC of the proposed staging system was 0.63 in the training set (SE 0.05) and 0.62 (SE 0.07) in the validation set, which indicated low discriminative power.
Discussion: Although bilateral second order biliary involvement, and vascular or lymph node involvement on preoperative imaging have predictive power for resectability of HCCA, they have inadequate discriminative power to form a staging system. No patients should be withheld from exploration based on these criteria.
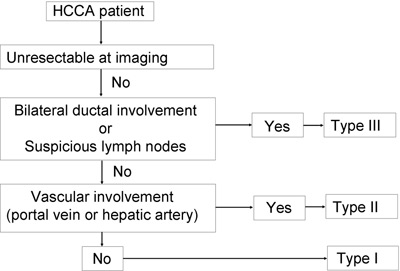 Figure 1. Proposed preoperative staging system to predict the chance of a R0 resection in HCCA.
Back to 2014 Annual Meeting Posters
|