|
Back to Annual Meeting Posters
Dissatisfaction After Laparoscopic Heller Myotomy
Sharona B. Ross*, Carrie E. Ryan, Benjamin L. Jacobi, Harold Paul, Kenneth Luberice, Paul Toomey, Alexander Rosemurgy
General Surgery, Florida Hospital Tampa, Tampa, FL
Introduction: Laparoscopic Heller myotomy alleviates symptoms of achalasia; however, we have observed a small subset of patients who are dissatisfied with their experience. This study was undertaken to identify causes of dissatisfaction after laparoscopic Heller myotomy and to identify predictors of dissatisfaction following myotomy.
Methods: With IRB approval, all patients undergoing laparoscopic Heller myotomy at our institution from 1992 to 2012 were prospectively followed. Using a Likert scale patients rated their frequency and severity of symptoms before and after myotomy. Patients graded their experience from "Very Satisfying" to "Very Unsatisfying". Objective outcomes were determined by esophagography / esophagoscopy. Complaints were derived from postoperative surveys, clinic visits, and phone surveys. Median data are reported.
Results: Of the 597 patients undergoing laparoscopic Heller myotomy, 44 (7%) patients reported some level of dissatisfaction following myotomy with follow-up at 32 months. Dissatisfied patients were more likely to have undergone prior abdominal operations (45% vs. 28%, p=0.03) and previous myotomies (16% vs. 5%, p=0.02). Dissatisfied patients also had longer postoperative lengths of stay (2 days vs. 1 day, p=0.01), generally because of postoperative complications or exacerbations of preoperative comorbidities. For dissatisfied patients, symptom frequency and severity persisted after myotomy and were more notable than for satisfied patients (p<0.03 for all; Figure).
Conclusions: Dissatisfaction is fortunately uncommon after laparoscopic Heller myotomy. Dissatisfaction is directly related to persistent severe and frequent symptoms; longer lengths of stay, previous abdominal operations, and "re-do" myotomies predict dissatisfaction. Patients with notable comorbidities and / or previous abdominal operations, particularly Heller myotomy, are more likely to be dissatisfied after laparoscopic Heller myotomy should be counseled preoperatively. Comorbidities should be addressed preoperatively and for patients with previous notable abdominal operations, particularly myotomy, alternatives to laparoscopic Heller myotomy should be considered.
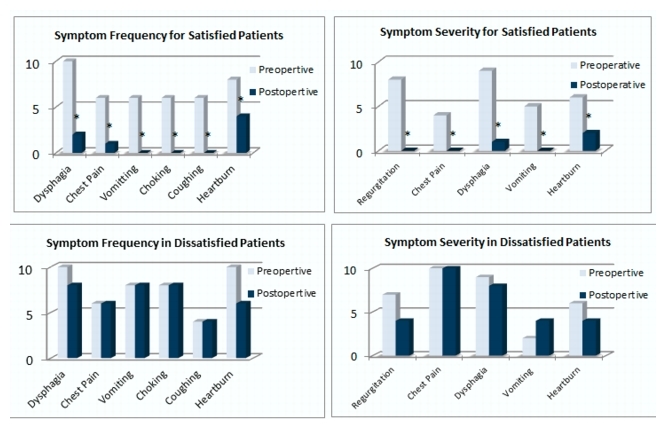
Figure depicts the disparity of symptom resolution between satisfied and dissatisfied patients. *denotes symptom improvement after myotomy (p < 0.05).
Back to Annual Meeting Posters
|

