|
Back to Annual Meeting Posters
Minimally Invasive Full Thickness Colonic Resection: a Novel Localised Excision Procedure
Adela Brigic*1, Paul D. Sibbons2, Chris H. Fraser1, Susan K. Clark1, Robin H. Kennedy1
1Department of Surgery, St. Mark's Hospital and Academic Institute, Harrow, United Kingdom; 2Northwick Park Institute for Medical Research, Northwest London Hospitals NHS Trust, Harrow, United Kingdom
Aims:
Worldwide introduction of the bowel cancer screening programmes has lead to an increase in the number of patients diagnosed with complex, benign colonic polyps unsuitable for endoscopic resection. A significant proportion is referred for hemicolectomy, which is associated with significant risk of morbidity and mortality. To address this and improve clinical outcomes, we modified a previously reported full thickness laparo-endoscopic excision (FLEX) technique developed in our institution.
Methods:
Following a series of ex-vivo experiments to standardise procedural steps, surgery was performed in five 70-kg pigs. A simulated colonic polyp was created by endoscopic injection of Spot® and the clearance margin was delineated by circumferential placement of mucosal argon plasma coagulator (APC) marks. Full thickness eversion of the colonic wall that contains the simulated lesion was achieved by endoscopic placement of prototype BraceBars (BBs). The everted segment was excised using a linear laparoscopic stapler placed below the BBs. The first pig was terminated immediately and others 8 days after surgery.
Results:
Procedure duration was defined from placement of mucosal APC marks to specimen excision with a median time of 26 min (range 20-31 min). All excised specimens contained three pairs of BBs delineating clearance margin with a median diameter of 5.1 cm (range 4.5-6.3 cm).
Postoperative recovery in survival animals was uneventful and post-mortem examination demonstrated well-healed resection sites with no evidence of intra-abdominal infection or inadvertent organ damage. Endoscopic evaluation of anastomoses at post-mortem examination excluded stenosis. Histological assessment of the partial circumferential anastomosis showed primary closure by mucosal abuttal and regeneration together with restoration of continuity of submucosa.
Conclusions:
This proof-of-concept survival study has demonstrated the feasibility of safely achieving full thickness colonic specimens exceeding 5 cm in diameter. Accurate placement of endoscopic BBs ensures completeness of excision, reducing the risk of recurrence or residual disease while laparoscopic overview avoids collateral damage.
This is the first localized excision technique described to date suitable for translational study in humans as an alternative to hemicolectomy. The ability to preserve mesenteric vasculature and colonic length is likely to result in less morbidity and mortality, reduced treatment costs and better functional outcomes.
Figure 1: Full-thickness colonic specimen with APC marks delineating clearance margin
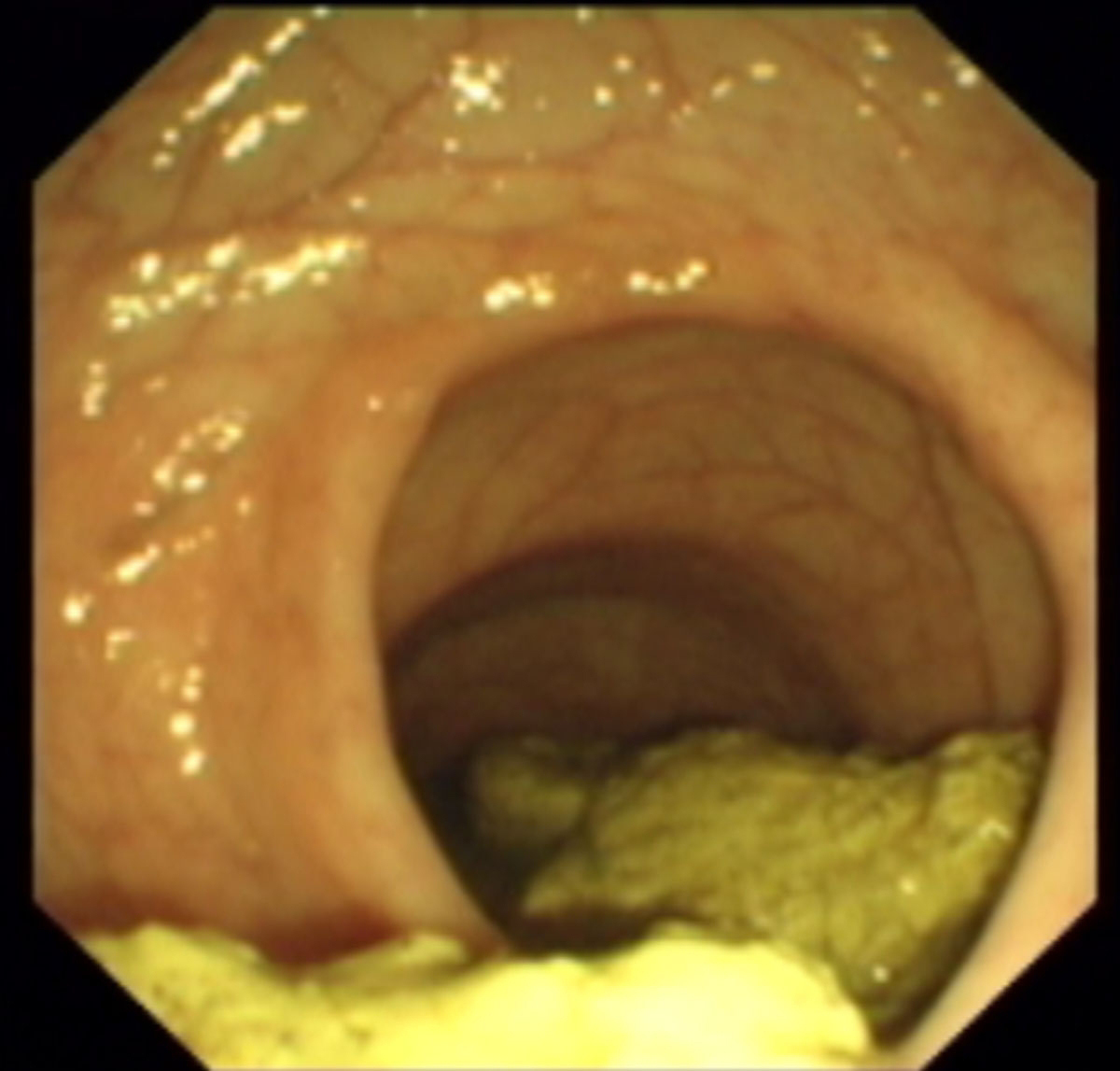 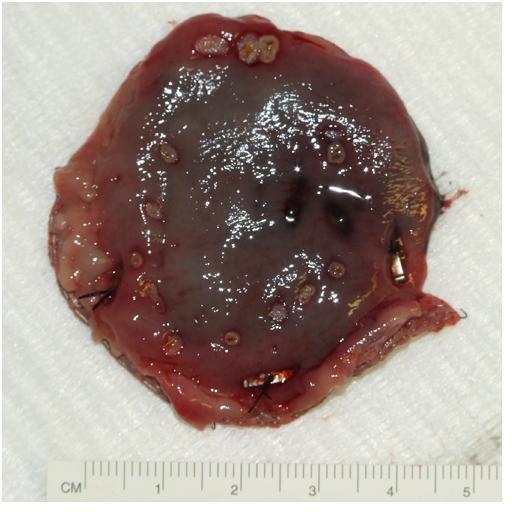
Figure 1: Full-thickness colonic specimen with APC marks delineating clearance margin
Figure 2: Endoscopic examination of the excision site 8 days post procedure
Back to Annual Meeting Posters
|

