
|
|
Back to Annual Meeting Posters
Clinical Profile and Skeletal Muscle Histopathology of Patients Affected With Early Diagnosed Colorectal Cancer: Diagnostic and Prognostic Markers of Disease?
Mario Gruppo*1, Nicoletta Adami2, Sandra Zampieri2, Roberto Rizzato1, Mario Bernardo3, Benedetto Mungo1, Renato Salvador1, Lino Polese1, Stefano Merigliano1
1Department of Surgical, Oncological and Gastroenterological Sciences, University Hospital of Padua, Padova, Italy; 2Department of Biomedical Sciences, University Hospital of Padua, Padova, Italy; 3Department of Emergency, Anaesthesiology and Intensive care, University of Tor Vergata, Rome, Italy
Background
Skeletal muscle in patients with cancer undergoes many morphological changes due to immuno-inflammatory factors of tumor origin and/or to the pharmacologic treatment of the disease. The latest event of these changes is cancer cachexia.
The aim of our study was to investigate the clinical characteristics and the histopathologic features of skeletal muscle and excised tumor from patients affected with colorectal cancer at diagnosis in order to possibly identify clinical factors associated to myopathic features that could be used as predictive biomarkers of disease progression.
Patients and methods
Morphometric studies and immunohistochemical analyses were performed on intraoperative rectus abdominis muscle biopsies from weight stable patients with an early diagnosis of colorectal cancer, before systemic or radiant therapies, with no signs of muscle weakness or myopathies. The correlation between histopathologic findings of skeletal muscle biopsies, resected tumor, and clinico-serological characteristics was investigated.
Results
44 patients and 17 controls affected with non-inflammatory benign diseases, were recruited for the study. In the skeletal muscle biopsies from cancer patients, we observed a subclinical myopathy characterized by an abnormal distribution of myonuclei relocated from the periphery inside the myofiber, and by the presence of regenerating muscle fibers. The percentage of myofibers with abnormally located myonuclei was significantly higher in patients (median= 9%) compared to controls (median= 2.7%) (p=0.0002). Moreover, the percentage of regenerating myofiber expressing the MHC-emb and N-CAM biomarkers was higher in patients compared to controls (MHC-emb positive 14,6 % vs 5,9% p=n.s; N-CAM positive 31,7 % vs 5,9%, p=0.04) (Tab I). No correlations were found between the histopathological findings of the skeletal muscle and clinico-serological characteristics of the patients. We found an inverse correlation between the number of abnormally nucleated myofibers and the presence of lymph node metastasis (N+) (ñ)=-0.64 (p=0.002). Myofibers atrophy wasn't observed. The ATPase analyses of skeletal muscle biopsies from patients and controls showed a higher percentage of fast type fibers in skeletal muscle biopsies from cancer patients compared to controls (56% vs 46%, p=0.06) (Tab. I). Interestingly, the internally nucleated myofibers were predominantly of fast type (Fig.1).
Conclusions
Patients affected with colorectal cancer display early signs of a subclinical myopathy, characterized by abnormally nucleated and regenerating myofibers, that is inversely associated with the presence of lymph node metastasis. Additional follow-up studies are needed to clarify this association, but our observation could provide new diagnostic biomarker of disease progression in specific subgroup of patients.
Table I Histopathological features of rectus abdominis muscle biopsies
| Patients | Controls | p | | Mean myofiber diameter (μm) | 51.1 | 50.3 | n.s. | | Abnormally nucleated myofibers (%) | 9 | 2.7 | 0.0002 | | Type II fibers (%) | 56 | 46 | 0.06 | | MHC-emb positive myofibers (%, no.) | 14.6 (6) | 5,9 (1) | n.s | | N-CAM positive myofibers (%, no.) | 31.7 (3) | 5,9 (1) | 0.04 |
MHC-emb embryonic myosin heavy chain; N-CAM neural cell adhesion molecule; n.s. not significant.
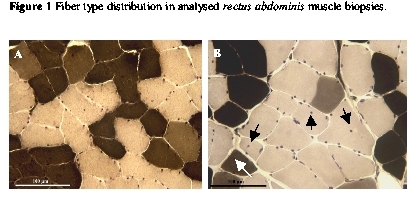
A and B: ATPase staining after preincubation at pH 4.35, of cross sections from control (A) and patient (B) muscle biopsies. Fast-type fibers are visualized as light, while slow-twitch fibers are dark. Fast fibers are predominant in cancer patients muscle biopsies and preferentially show internal nuclei (arrowhead). Calibration bar=100 µm.
Back to Annual Meeting Posters
|

